|
Introduction
Microsporidia
is a family of very rare, spore-forming organisms
which tend to infect humans and animals. It was
earlier classified under protozoans but has now
been reclassified as fungi. Although a large
family of 1,300 formally described species in 160
genera, only 13 species have been known to cause
human disease.(1) These organisms most commonly
involve the gastrointestinal tract followed by
infection of the cornea, which is relatively rare,
accounting for 0.4% of total cases presenting with
keratitis. (2)
Case Presentations
Case 1
A 55 year old male patient, presented to the
ophthalmology OPD with complaints of watering,
irritation, redness and pain in the left eye since
10 days. He was not a known case of diabetes
mellitus, HIV or tuberculosis. He denied any
history of previous trauma and any similar
complaints in the past. He had no history of
fever. He had no history of similar complaints in
the family.
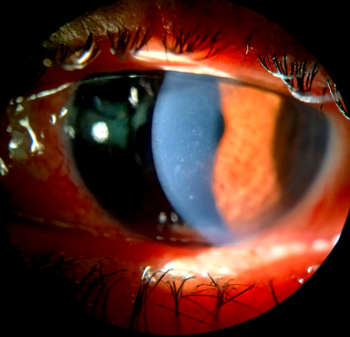
On examination, right eye was normal, left eye
examination showed edematous lids, circumcorneal
congestion on conjunctiva and corneal sensations
were intact [Fig 1]. Pupil reaction was sluggish.
Cells and flare were seen in the left eye.
Anterior chamber was quiet on examination.

|
| Fig
1: Left eye showing edematous lids and
circumcorneal congestion |
Case 2
A 42 year old male
patient, came to the ophthalmology OPD with
similar complaints of redness and irritation in
the left eye since 7 days. He had no history of
trauma to the eye. He was not a known case of
diabetes mellitus, HIV or tuberculosis and had no
similar complaints in the past. No similar
complaints in the family were found.
On examination right
eye was normal. Left eye examination showed
congestion on conjunctiva and mild discharge.
Slit lamp
examination was performed in both patients which
revealed coarse, raised punctate epithelial
lesions with a typical stuck on appearance
[Fig-2].
Corneal scrapings
from both patients were sent to microbiology
laboratory for staining and cultures.
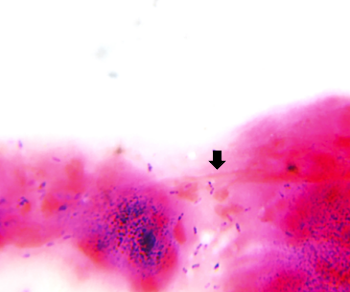
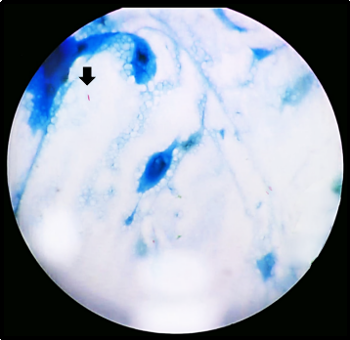
On microscopy Gram
stain showed plenty of inflammatory debris along
with violet colored ovoid spores resembling Microsporidia
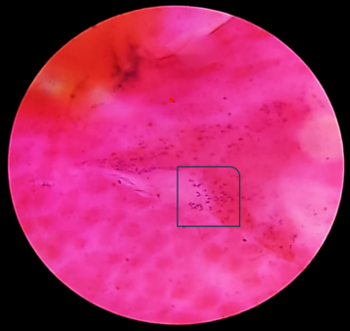
(Fig 3.a, 3.b). On Giemsa stain, deep blue oval
spore like structures were seen (Fig 3.c.).
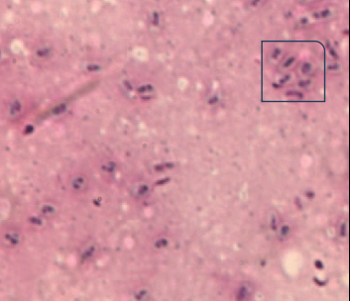
Modified Acid fast stain (1% H2SO4)
showed acid fast, bright red spores against blue
background (Fig 3.d). On slit lamp examination
stuck on appearance in corneal stroma was seen.
Culture was done on
Blood agar, MacConkey agar and Sabouraud dextrose
agar which yielded no growth.
|
Fig 2: Slit lamp
examination revealing typical stuck on
appearance |
|
|
| Fig
3a: Gram-stained smear showing
violet-colored ovoid spores suggestive of
Microsporidia (Gram stain, ×1000
magnification). |
Fig
3b: Gram stained smear showing violet
colored ovoid spores resembling Microsporidia
(Gram stain, ×1000 magnification) |
|
|
| Fig
3c: Giemsa-stained smear showing deep blue
oval spore-like structures suggestive of Microsporidia
(Giemsa stain, ×1000 magnification). |
Fig
3d: Modified Acid fast stained smear
showing acid fast, bright red spores
against blue background (Modified acid
fast, ×1000 magnification) |
Differential
diagnosis: The cases of Microsporidial
keratitis are quite difficult to diagnose as they
resemble viral and fungal keratitis. Thorough
investigations along with clinical findings aid in
confirming the diagnosis which in turn helps to
initiate appropriate therapy. The findings in
these two cases along with the investigation
reports strongly suggested Microsporidial
keratitis.
Treatment and
follow-up: The patients were started on
fluconazole eye drops for 6 days, three times
daily along with moxifloxacin eye ointment which
had to be applied before bedtime. Patients were
reviewed after 3 days of starting therapy and were
symptomatically better and cornea was found to be
clear.
Discussion
Microsporidial
keratitis is increasingly recognized as an
emerging cause of infectious keratitis and has
gained considerable attention in recent years.
Traditionally, Microsporidia were regarded
as opportunistic pathogens that primarily affected
immunocompromised individuals, particularly those
with human immunodeficiency virus infection.(3)
However, recent literature suggests a changing
epidemiological trend, with a growing number of
cases now being reported among immunocompetent
individuals without identifiable systemic risk
factors.(4) The present cases further support this
observation, as both patients were immunocompetent
and had no associated systemic illness or known
ocular predisposing factors.
Clinically,
microsporidial keratitis may present with a broad
spectrum of manifestations ranging from
superficial punctate keratoconjunctivitis to
deeper stromal keratitis.(5) Because of this
variability, the condition may easily mimic other
forms of infectious keratitis, particularly viral
or fungal keratitis, which often leads to delays
in diagnosis and appropriate management.(2)
Several studies have described the presence of
coarse granular or “stuck-on” appearing stromal
infiltrates as an important clinical clue
suggestive of microsporidial infection.(6)
Although this feature is not pathognomonic, its
presence in unilateral, non-resolving keratitis
should prompt clinicians to consider
microsporidial infection in the differential
diagnosis.(7)
Accurate diagnosis
of microsporidial keratitis relies largely on
microbiological confirmation. Conventional
staining techniques such as Gram staining and
modified acid-fast staining remain useful and
practical methods for identifying the
characteristic oval or ovoid spores of Microsporidia
in corneal scrapings.(8) These techniques are
particularly valuable in resource-limited settings
where advanced diagnostic tools may not be readily
available.(9) Although newer diagnostic modalities
such as polymerase chain reaction (PCR), in vivo
confocal microscopy, and metagenomic sequencing
offer improved sensitivity and allow species-level
identification, their use is often limited to
specialized laboratories.(10)
Management of
microsporidial keratitis continues to evolve with
increasing awareness of the disease. Various
therapeutic approaches have been described,
including the use of topical antimicrobial agents
such as voriconazole, fumagillin, and other azole
antifungals.(11) In the present cases, both
patients demonstrated a favorable clinical
response following initiation of topical
fluconazole therapy, which is consistent with
outcomes reported in recent literature.(12) Early
initiation of appropriate therapy is essential, as
delayed diagnosis or inadvertent use of topical
corticosteroids may worsen the infection and
prolong the disease course.(13)
Despite increasing
recognition, microsporidial keratitis remains
under diagnosed due to its nonspecific clinical
presentation and overlap with other infectious
keratitis. Maintaining a high index of suspicion
in cases of unilateral, non-resolving keratitis
that do not respond to routine antibacterial or
antiviral therapy is therefore essential for early
diagnosis and timely management.
References
- Chander J. Microsporidiosis. In Chander J,
editor. Textbook of medical mycology. 4th ed.
New Delhi: Jaypee Brothers Medical Publishers;
2018. p. 494-501.
- Chou TY, Bansal J, Seidman R, et al. Bilateral
microsporidial keratoconjunctivitis in a
clinically healthy female receiving intravitreal
steroid injections: associations and potential
risk factors. Am J Ophthalmol Case Rep.
2022 Jul 9;27:101659.
- Moshirfar M, Somani SN, Shmunes KM, et al. A
narrative review of microsporidial infections of
the cornea. Ophthalmol Ther. 2020;9(2):265-278.
- Mohanty A, Sahu SK, Sharma S, et al. Past,
present, and prospects in microsporidial
keratoconjunctivitis: a review. Ocul Surf. 2023
Apr;28:364-377.
- Matoba A, Goosey J, Chévez-Barrios P.
Microsporidial stromal keratitis:
epidemiological features, slit-lamp
biomicroscopic characteristics, and therapy. Cornea.
2021 Dec 1;40(12):1532-1540.
- Mohanty A, Behera HS, Barik MR, et al. Microsporidia-induced
stromal keratitis: a new cause of presumed
immune stromal keratitis. Br J Ophthalmol. 2023;107(5):607-613.
- Alkatan HM, Al-Zaaidi S, Athmanathan S.
Microsporidial keratitis: literature review and
report of 2 cases in a tertiary eye care center.
Saudi J Ophthalmol. 2012
Apr;26(2):199-203.
- Sharma S, Das S, Joseph J, et al.
Microsporidial keratitis: need for increased
awareness. Surv Ophthalmol. 2011
Jan-Feb;56(1):1-22.
- Donthineni PR, Murthy SI, Joseph J, et al.
Microsporidial stromal keratitis: an uncommon
etiology of bilateral simultaneous corneal
infection. Asian J Ophthalmol. 2020;17(3):311-317.
- Ghenciu LA, Faur AC, Bolintineanu SL, et al.
Recent advances in diagnosis and treatment
approaches in fungal keratitis: a narrative
review. Microorganisms. 2024;12(1):161.
- Ramatchandirane B, Kumar MA, Marimuthu Y, et
al. Successful treatment of microsporidial
keratoconjunctivitis (MKC) with a combination of
topical voriconazole 1% and gatifloxacin 0.5%: a
large case series of 29 patients. Cureus. 2023
Nov 22;15(11):e49247.
- Devi L, Prajna NV, Srinivasan M, et al.
Microsporidial infection masquerading as graft
rejection post-Descemet's stripping automated
endothelial keratoplasty. Indian J
Ophthalmol. 2017 Sep;65(9):869-871.
- Mohanty A, Kelgaonkar A, Behera HS, et al. Microsporidia-associated
anterior uveitis after keratoconjunctivitis. Cornea.
2023 Nov 1;42(11):1439-1445.
|




