|
Introduction
Health
is one of the key components of human capital
which is crucial for economic development of any
country. In developing countries like India,
public health expenditure plays a critical role in
improving population health and reducing mortality
rates. Despite fast economic growth, India
continues to face challenges such as high infant
mortality and maternal mortality rates. Government
spending on health is expected to improve health
outcomes through enhanced infrastructure,
availability of medical personnel, and improved
access to healthcare services. While arguing in
favour of the public health spending reported that
there are various positive externalities
associated with health (1). Apart from this,
social factors such as female literacy also
influence health outcome by influencing health
awareness, maternal care practices and utilization
of healthcare facilities. Literature studying the
impact of public health expenditure on health
outcome is limited. Therefore, it is very
important to assess the relationship between
public health expenditure and health outcome. Such
assessment helps in implementing health policies
in developing countries like India. In India,
public health expenditure has historically lagged
behind global norms, often hovering around 1-1.5%
of GDP, compared to the WHO’s recommended 5% of
GDP. Over the last three decades India has
undertaken various reforms and increased
government spending on health infrastructure,
immunization programmes and maternal and child
health services. Understanding how these
expenditures translate into measurable outcomes is
critical for policy makers.
Previous literature
investigating the linkage between public health
expenditure and health outcome reports
inconclusive results. For example, studies
investigated the impact of public health
expenditure on infant mortality rate using an
unbalanced panel of 31 states and UTs in India
from 1984-2012 (2) reported that public health
expenditure helps in reducing IMR. Another study
reported that public health expenditure does not
have significant effect on mortality rates in
India (3). Despite the prior results one thing is
clear that public expenditure may improve health
outcome (4). Hence, an empirical assessment is
needed to check the impact of public health
expenditure on health outcome. The inconsistency
in findings of earlier research led the researcher
to empirically investigate the relationship
between public health expenditure and health
outcome using time series data from 1990-2024. The
objective of the study is to investigate the
impact of public health expenditure on health
outcome. Three key indicators such as MMR, IMR and
Life expectancy are used as dependent variable to
measure health outcome. However, along with public
health expenditure, other factors such as GDP per
capita, and female literacy are also included in
the study.
Data and Methodology
The study is based
on secondary data sources. The required data for
the period from 1990-2024 was extracted from World
Development Indicators which is available online
on the World Bank website. Health outcome was
measured by using infant mortality, maternal
mortality and life expectancy. Three separate
models have been specified for each of the
above-mentioned variables measuring health outcome
as dependent variable. Independent variables are
GDP per capita (US $), public health expenditure
per capita (US $) and female literacy.
To meet the
objective of the study, the following models has
been specified.
Model-1
IMRt = f (GDPt, HEt, FLt) ……………………………………………..(1)
Model-2
MMRt = f (GDPt, HEt, FLt) ……………………………………………(2)
Model-3
LEt = f (GDPt, HEt, FLt) ……………………………………………….(3)
Where IMR is infant mortality rate, HE represents
health expenditure and FL is the female literacy
rate. All the variables were transformed into log
form. Hence the log linear based models can be
expressed as:
lnIMRt= β0 + β1(lnGDPt)
+ β2(lnHEt) + β3(lnFLt)
+ έt (Model-1)
lnMMRt= β0 + β1(lnGDPt)
+ β2(lnHEt) + β3(lnFLt)
+ έt (Model-2)
lnLEt= β0 + β1(lnGDPt)
+ β2(lnHEt) + β3(lnFLt)
+ έt (Model-3)
Where, βs are coefficients of
dependent variables, έ is the error term and t
denote time series.
In order to examine
the long run relationship among the study
variables, the Autoregressive Distributed Lag
(ARDL) Bound Test approach has been adopted.
Before selection of the ARDL model, Augmented
Dickey-Fuller (ADF) unit root test has been
conducted to check the stationarity of the study
variables. The results of the unit root test
demonstrates that the variables under study have
mixed I(0) and I(1) order of integration as shown
in table 1. Given this the ARDL approach was
chosen for the study.
Our models in ARDL form will be expressed as
under
ΔlnIMRt = α0 + β1lnIMRt-1
+ β2lnGDPt-1 + β3lnHEt-1
+ β4lnFLt-1 + j
ΔlnIMRt-j + k ΔlnGDPt-k
+ l ΔlnHEt-l + m ΔlnFLt-m
+ μt
ΔlnMMRt = α0 + β1lnMMRt-1
+ β2lnGDPt-1 + β3lnHEt-1
+ β4lnFLt-1 + j
ΔlnMMRt-j + k ΔlnGDPt-k
+ l ΔlnHEt-l + m ΔlnFLt-m
+ μt
ΔlnLEt = α0 + β1lnLEt-1
+ β2lnGDPt-1 + β3lnHEt-1
+ β4lnFLt-1 + j
ΔlnLEt-j + k ΔlnGDPt-k
+ l ΔlnHEt-l + m ΔlnFLt-m
+ μt
Where α0 is a constant, μt
is the error term.
Trends of Public Health Expenditure and
Health Outcome during 1990-2024
|
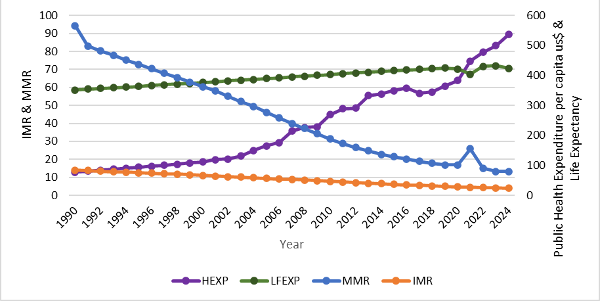
| Figure
1: Trends of Public Health Expenditure,
IMR, MMR and Life Expectancy from
1990-2024 [Source: World Bank Data] |
The trends of public
health expenditure, infant mortality rate,
maternal mortality rate, life expectancy in India
are shown in Figure 1. It shows that public health
expenditure was stagnant up to 2004 and then
started an increasing trend. IMR has shown a
downward trend from 84.3 to 23.6 per thousand live
births during this time. MMR also shows a downward
trend from 566 per lakh live births to 80 during
1990-2024. Life Expectancy shows a gradual
increasing trend from 58.62 years to 70.62 years
during the time period under study. A preliminary
observation of the trendlines shows that there is
a positive relationship between health expenditure
with life expectancy and negative relationship
with infant mortality and maternal mortality.
Results and Discussion
Table 1 shows the
results of the ADF test for unit root and it was
found that the variables infant mortality,
maternal mortality and health expenditure are
stationary at level and variables, Life
Expectancy, GDP per capita and Female Literacy are
stationary at levels.
|
Table 1: Results of ADF Test
|
|
Variables
|
At Level
|
At First Difference
|
Decision
|
|
t- statistics
|
P-value
|
t- statistics
|
P- value
|
|
lnIMR
|
-5.455421
|
0.0005***
|
-
|
-
|
I(0)
|
|
lnMMR
|
-3.949811**
|
0.0254
|
|
|
I(0)
|
|
lnGDPpc
|
-2.075498
|
0.5386
|
-4.106893**
|
0.016
|
I(1)
|
|
lnHE
|
-4.759460***
|
0.0040
|
-
|
-
|
I(0)
|
|
lnFL
|
-2.918340
|
0.1700
|
-177.0280***
|
0.000
|
I(1)
|
|
lnLE
|
4.072376
|
1.0000
|
-0.4553649***
|
0.005
|
I(1)
|
|
** indicates the significance level of 5%
and *** indicate the significance level of
1%.
|
ARDL Bound test
F-statics was used at the first stage to
investigate the long-run relationship among the
variables. The results of ARDL Bound test (Table
2) for dependent variable lnIMR shows that the
F-statistic value is greater than the upper bound
I(1) value at 5% level of significance. This means
that there is cointegration among the variables in
the model. In Model-2 (lnMMR as dependent
variable) and Model-3 (lnLE as dependent variable)
the ARDL bound test shows F-statistic value for
both the models is less than the upper bound value
at 5% level of significance. This clearly
indicates that there is no long-run relationship
exists among the variables when lnMMR and lnLE are
treated as dependent variable. The diagnostics
test shows no issues with serial correlation,
heteroscedasticity and normality of residuals. The
Ramsey Reset test results for stability of the
model is insignificant at 5% level.
|
Table 2: Results of Bound Test (Dependent
variable lnIMR)
|
|
Model-1
|
F-stat
|
Critical value
|
Diagnostic test
|
|
Significance level
|
I(0)
|
I(1)
|
J-B test-p=0.699
LM test-p=0.391
BPG Hetero-p=0.8107
Ramsey Reset test, p=0.1013
|
|
lnIMR|lnGDP|lnHE|lnFL
|
9.87
|
1%
|
5.17
|
6.36
|
|
5%
|
4.01
|
5.07
|
|
10%
|
3.47
|
4.45
|
|
Table 3: Results of Bound Test (Dependent
variable lnMMR)
|
|
Model-2
|
F-stat
|
Critical value
|
Diagnostic test
|
|
Significance level
|
I(0)
|
I(1)
|
J-B test-p=0.587
LM test-p=0.096
BPG Hetero-p=0.5148
Ramsey Reset test, p=0.710
|
|
lnMMR|lnGDP|lnHE|lnFL
|
3.22
|
1%
|
5.17
|
6.36
|
|
5%
|
4.01
|
5.07
|
|
10%
|
3.47
|
4.45
|
|
Table 4: Results of Bound Test (Dependent
variable lnLE)
|
|
Model-3
|
F-stat
|
Critical value
|
Diagnostic test
|
|
Significance level
|
I(0)
|
I(1)
|
J-B test-p=0.905
LM test-p=0.321
BPG Hetero-p=0.522
Ramsey Reset test, p=0.416
|
|
lnLE|lnGDP|lnHE|lnFL
|
3.67
|
1%
|
5.17
|
6.36
|
|
5%
|
4.01
|
5.07
|
|
10%
|
3.47
|
4.45
|
|
Table 5: Results of Long-run
relationship: Dependent variable lnIMR
|
|
Variable
|
Coefficient
|
Std Error
|
t- statistic
|
Prob.
|
|
lnGDPpc
|
0.750482
|
0.402412
|
1.864959
|
0.0819
|
|
lnHE
|
-0.271582
|
0.188000
|
-1.444583
|
0.1691
|
|
lnFL
|
0.471459
|
0.467789
|
01.007846
|
0.3295
|
Table 5 shows
results of long-run relationship. Results reveal
that although the ARDL bounds test confirms the
existence of a long-run relationship among the
variables, the estimated long-run coefficients are
statistically insignificant at the 5 percent
level. This suggests that while the variables move
together in the long-run, none of the individual
explanatory variables exerts a statistically
significant independent influence on the dependent
variable. Previous research reported that there is
no significant effect of current public health
expenditure on mortality rates in India during the
period from 1980-1999(3). The finding of the study
replicates the same during the period from
1990-2024 in the long run relationship between the
variables.
|
Table 6: Results of Short-run
relationship: Dependent variable lnIMR
|
|
Variable
|
Coefficient
|
Std Error
|
t- statistic
|
Prob.
|
|
D(lnGDP)
|
0.047642
|
0.007731
|
6.162087
|
0.0000
|
|
D(lnGDP) (-1)
|
-0.011999
|
0.004369
|
-2.746370
|
0.0150
|
|
D(lnGDP) (-2)
|
-0.051468
|
0.007065
|
-7.284520
|
0.0000
|
|
D(lnHE)
|
0.014476
|
0.005013
|
2.887508
|
0.0113
|
|
D(lnHE) (-1)
|
0.050539
|
0.009025
|
5.600066
|
0.0001
|
|
D(lnHE) (-2)
|
0.037050
|
0.007161
|
5.173611
|
0.0008
|
|
D(lnFL)
|
-0.472521
|
0.112342
|
-4.206088
|
0.0008
|
|
C
|
-0.469377
|
0.068112
|
-6.891270
|
0.0000
|
|
T
|
-0.009235
|
0.001421
|
-6.499764
|
0.0000
|
|
ECM(-1)
|
-0.111189
|
0.016157
|
-6.881856
|
0.0000
|
The results of
short-run relationship for model-1 is shown in
Table 6. Results reveal that the lagged ECM is
highly significant confirming long-run relation in
the model. This is a clear indication that any
short run deviations from equilibrium is adjusted
to long run at 11 percent annually. Further it was
seen that in the short run, one percent increase
in GDP contributes 40 percent to health outcome as
the coefficient is highly significant at 1% level.
Likewise, one percent increase in health
expenditure contributes 10% to health outcome
(IMR). Also, one percent increase in female
literacy contributes 47% to health outcome.
Table 7 demonstrates
the short run relationship with dependent variable
MMR. Results revealed that GDP in current period
and lag (1) is significant at 5% level. Similarly,
previous health expenditure lag (1) significantly
affects MMR. Likewise, female literacy is also
significantly contributed to reduction in MMR.
|
Table 7: Results of Short-run
relationship: Dependent variable lnMMR
|
|
Variable
|
Coefficient
|
Std Error
|
t- statistic
|
Prob.
|
|
D(lnGDP)
|
0.641642*
|
0.254562
|
2.520568
|
0.0235
|
|
D(lnGDP) (-1)
|
-1.719587
|
0.336334
|
-5.112742
|
0.0001
|
|
D(lnHE)
|
0.281758
|
0.187054
|
1.506288
|
0.1528
|
|
D(lnHE) (-1)
|
1.248288
|
0.317961
|
3.925908
|
0.0013
|
|
D(lnHE) (-2)
|
0.625939
|
0.307415
|
2.036139
|
0.0598
|
|
D(lnFL)
|
-9.554647
|
2.906921
|
3.286861
|
0.0050
|
|
C
|
9.126609
|
2.398411
|
3.805273
|
0.0017
|
|
T
|
-0.061851
|
0.017301
|
-3.574895
|
0.0028
|
Table 8 portrays the
results of model-3 where Life expectancy is
treated as dependent variable in examining the
relationship between public health expenditure and
health outcome. The results reveal that GDP in
current period and lag (1) is significant at 5%
level. Similarly, current and previous health
expenditure lag (1) significantly affect life
expectancy. Likewise, female literacy is also
significantly contributed to improvement in life
expectancy.
|
Table 8: Results of Short-run
relationship: Dependent variable lnLE
|
|
Variable
|
Coefficient
|
Std Error
|
t- statistic
|
Prob.
|
|
D(lnGDP)
|
0.593841
|
0.021599
|
-2.749336
|
0.0137
|
|
D(lnGDP) (-1)
|
0.142463
|
0.033804
|
4.214338
|
0.0006
|
|
D(lnHE)
|
0.047072
|
0.016377
|
-2.874339
|
0.0105
|
|
D(lnHE) (-1)
|
0.103403
|
0.021794
|
-4.744519
|
0.0002
|
|
D(lnHE) (-2)
|
0.045808
|
0.022424
|
-2.042837
|
0.0569
|
|
D(lnFL)
|
1.219542
|
0.577683
|
-2.111091
|
0.0499
|
|
C
|
2.988164
|
0.700285
|
4.267066
|
0.0005
|
|
T
|
-0.006491
|
0.001155
|
-5.620629
|
0.0000
|
Overall, the results
reveal that public health expenditure has a
statistically significant impact on health
outcomes (in the short-run), highlighting the
importance of sustained public investment in the
healthcare sector. In contrast, female literacy
exhibits a significant effect in the short-run,
suggesting that improvements in women’s education
rapidly influence health related behaviours and
outcomes. The findings of the study are in line
with findings of the earlier research (2,4,5).
Conclusion
The empirical
results of the study show that public health
expenditure has a positive and significant effect
on life expectancy and negative and significant
effect on IMR and MMR. The findings of the study
have important policy implications. Public health
expenditure plays a crucial role in improving
overall health outcome of the country. Previous
research opined that low level of public spending
might be one of the possible reasons of low
performance in health indicators in India(7).
Human Development Report, 2024 reflects that life
expectancy has increased from 58.6 in 1990 to 72
years in 2023. This progress is attributed to
national health programmes like National Health
Mission, Ayushman Bharat, Janani Suraksha Yojana
and Poshan Abhiyaan. This implies that public
healthcare expenditure plays a critical role in
improving health outcomes in India. But India
still falls in the medium human development
category in HDI ranking with HDI value 0.685 but
it is impressive that India is slowly approaching
towards high human development category. To
achieve this target the country, need to enhance
investment in public health expenditure and
improvement in health infrastructure.
References
- Self S, Grabowski R. How effective is public
health expenditure in improving overall health?
A cross-country analysis. Applied Econ.
2003;35(7): 835-845.
- Barenberg AJ, Basu D, Soylu C. The effect of
public health expenditure on infant mortality:
evidence from a panel of Indian states, 1983-84
to 2011-2012. J Development Stud.
2017; 53(10): 1765-1784.
- Deolalikar AB. Attaining the millennium
development goals in India: reducing infant
mortality, child malnutrition, gender
disparities and hunger-poverty and increasing
school enrolment and completion. Oxford
University Press; 2005.
- Farag M, Nandakumar AK, Wallack S, Hodgkin D,
Gaumer G, Erbil C. Health expenditures, health
outcomes and the role of good governance. Int
J Health Care Finance and Economics.
2013;13(1): 33-52.
- Mohanty RK, Behera DK. How effective is public
health care expenditure in improving health
outcome? an empirical evidence from the Indian
states [working paper]. New Delhi: National
Institute of Public finance and Policy; 2020.
- Bhalotra S. Spending to save? State health
expenditure and infant mortality in India. Health
Econ. 2007;16(9): 911-928.
- Rao MG, Choudhury M. Healthcare financing
reforms in India [working paper] New Delhi:
National Institute of Public Finance and Policy;
2012.
|




