|
Introduction
Radius
is a long bone located on the lateral side of
forearm. The shaft widens rapidly toward the
distal end, which is shallow anteriorly [1]. The
proximal and distal ends of radius are commonly
susceptible to trauma. Approximately 2-6% of
fractures occur at the proximal end and the neck
of radius, while the distal end fractures account
for about 8-20% of radius fractures and more
commonly seen in geriatric population [2].
However, distal end fractures are prevalent across
all age groups, but the pediatric and elderly
populations are considered at high risk.
Various studies have
shown that up to 25% of fractures in children
involve the distal end of the radius [3].
Adolescents are at higher risk due to a
significant gap between skeletal growth and
mineralization during puberty that may increase
fragility with additional cortical porosity of
radius and metaphysis[4]. The incidence of lower
end fractures has been rising recently in elder
population, largely due to an increasing number of
falls among the elderly people accounting for up
to 18% of all fractures in over 65 age group
[5].Among the women population, postmenopausal
women are particularly at risk because of calcium
deficiency and decreased bone density associated
with osteoporosis[6] and urban woman having 30%
greater risk than rural women[7]. There are
different types of distal radius fractures
including Colles’ fracture which is a metaphyseal
injury of the cortico-cancellous junction,
characterized by dorsal tilt, shift, and impaction
which occurs most commonly in elderly people.
Smith's fractures involve palmar tilt, wrist joint
injury involved Barton's fracture involved dorsal
aspect of articular surface and Chauffer's
fracture is an intra-articular fracture of radial
styloid [8].
Apart from
fractures, distal end of the radius is a common
site for aggressive malignant tumor and it is
treated by endoprosthesis, where correct surgical
technique is essential for the desired outcome
[9]. Following surgery, reduction in the radius
length along with the altered palmar tilt causes
considerable loss of movements in the forearm and
wrist joint with decreased grip strength [10,11].
Indian studies in the Sindhudurg and Konkan
regions of Maharashtra State show that
approximately 39.9% of wrist fractures are treated
surgically, which incurs considerable expenses
[12]. Some studies have shown the concave shape of
the anterior se distal radius and its angle
relative to the plate design. However, there is
still a lack of comprehensive morphological
information regarding the anterior and inferior
surfaces of the lower end of the radius [13-15].
While many morphological studies on the radius
exist in the fields of forensic anthropology and
orthopaedics, they often rely on radiographic
images, where soft tissue shadows or angulation
during imaging can alter the measured values [16].
A study on the
morphology of the lower end of radius and its
variations in Indian ethnicity is scarce.
Therefore, it is necessary to review surgical
methods for the distal part of the radius and
carefully consider the shape of the anterior and
inferior articular surfaces. A thorough
understanding of the bony architecture,
measurements, and their variations is crucial for
designing various prosthetic plates,
reconstructing the radio carpal joint and reducing
post-surgical complications in wrist fracture
surgery [17].
Aim and Objective
Aim: To analyse the
morphology and morphometric features of distal end
of radius for understanding their clinical
implications in orthopedic practice.
Objective: The following
parameters were studied morphologically and
morphometrically.
a. Length of styloid process of radius.
b. Shape of lateral and medial facet of inferior
articular surface of distal radius.
c. Circumferential diameter of distal end of
radius.
Methods
The descriptive
cross sectional study among 110 human dry radius
bones which were segregated into 55 right and 55
left sides from the Department of Anatomy were
used for the study. The study was approved by
Institutional Ethical Committee, Vinayaka
Mission’s Kirupananda Variyar Medical College and
Hospitals, Salem, Tamil Nadu, India. The equipment
used were vernier calipers, inelastic thread,
measuring scale and digital photography camera.
The following
parameters were measured on both right and left
side:
a. Length of
styloid process of radius: It was
measured by using vernier caliper from tip of the
styloid process to the lower vertical line of
anterior border of radius bone (Fig: 1)

|
|
Fig
1: Measurement of length of Styloid
Process of Radius (from the end of the
anterior border to the tip of styloid
process)
|
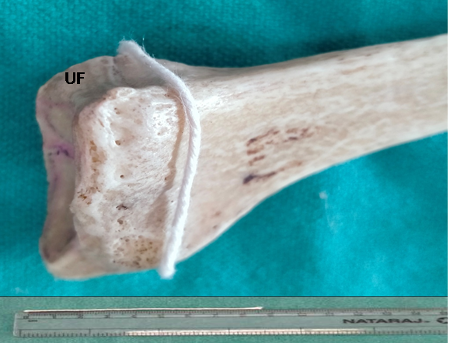
Fig
2: Measurement of Circumferential Diameter
of Distal End of Radius (Encircle the
thread 1cm above the upper margin of ulnar
facet (UF) and measure circumferential
diameter) |
b.
Circumferential diameter of lower end of radius:
It was measured by using an inelastic thread
surrounding 1cm above the upper margin of ulnar
notch of radius and thread was measured with
normal ruler. (Fig: 2)
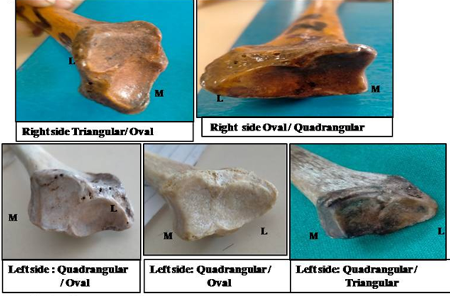
c. Shape of
inferior articular facet of radius: All
different shapes were documented (Fig: 3)
|
Fig
3: Various Shapes of Inferior Articular
Facet (M=Medial, L=Lateral
|
d. Any
abnormal bony variations in architecture were
documented.
Inclusion
criteria: Radius bones with intact
lower end.
Exclusion
criteria: Deformed and damaged lower
end of radius bones.
Statistical
Analysis:
Statistical
parameters were analyzed with ‘SPSS software 16’.
Standard deviation, mean values and the range were
calculated from the obtained results. Paired
sample t’ test was used to differentiate
morphometric values between the right and the left
sides of lower end of radius
Results
The mean length of
the styloid process of the right side was 1.15cm,
SD ± 0.16 cm with the variance of 0.03cm whereas
the mean length of left side was 1.10cm, SD ±
0.14cm and variance was 0.02cm.
|
Table 1:
Circumferential Diameter of Distal End
of the Radius
|
|
Right side
|
Left side
|
|
Mean
|
08.70 cm
|
08.47 cm
|
|
Minimum
|
07.30 cm
|
06.60 cm
|
|
Maximum
|
10.30 cm
|
09.90 cm
|
|
Std.Dev
|
0.73 cm
|
0.75 cm
|
|
Variance
|
0.53 cm
|
0.56 cm
|
The mean
circumferential diameter of right side was 8.70 cm
SD ± 0.73cm and maximum and minimum mean
circumferential diameter of right side were
10.30cm and 7.30 cm respectively. The mean
circumferential diameter of left side was 8.47cm
SD ± 0.75cm and maximum and minimum mean
circumferential diameter of left side were 9.90cm
and 6.60cm respectively.
The Shape of
inferior articular facet in the inferior articular
surface of distal radius varied from quadrangular
in the medial facet (R = 92% L = 98%), triangular
(R = 67 % L = 96 %) and oval (R = 32% L = 5.4 %)
in the lateral facet.
Discussion
The distal end of
radius is anatomically important as it forms wrist
joint with scaphoid and lunate bones. It maintains
the vertical position and supports the movements
of forearm and hand [1]. The body weight is
directly transmitted from the wrist joint to the
radius, making the anatomy of the lower end of the
radius of great clinical significance [18].
Fractures being common in the distal end[19].
Fractures are treated conservatively, but unstable
fractures need surgical treatments, and proper
positioning of the various components of the
distal end of the radius during surgery is crucial
to restoring normal wrist joint function, as
improper positioning can lead to disability [20].
With proper diagnosis and treatment, satisfactory
outcomes can be achieved even in severe injuries
[21]. Therefore, knowledge of the anatomy of the
distal articular surface of the radius is
important for radiologists, oncologists and
orthopaedic surgeons for accurately diagnosing
clinical conditions affecting this region and in
planning traumatic wrist surgeries.
In the present
study, the mean length of the styloid process on
the right side was found to be longer than on the
left side which contrasts with findings in the
Nepalese population, where the left side is longer
than the right [22]. In the present study are in
accordance with previous Indian studies,
suggesting that clinicians should consider these
values when performing wrist surgeries for
fractures and designing prosthesis plates for the
Indian population[20,24].
|
Table 2: Length of Styloid
Process of Radius – Right and Left
(Paired Samples t’ Test)
|
|
Paired Differences
|
T
|
df
|
Sig. (2-tailed)
|
|
Mean
|
Std. Deviation
|
Std. Error Mean
|
95% Confidence Interval of the Difference
|
|
Lower
|
Upper
|
|
.04681
|
.18749
|
.02735
|
.10186
|
.00824
|
1.712
|
46
|
0.104
|
In the present study
distal end circumference diameter was 8.70 ± 0.73
cm on the right side and 8.47 ± 0.73 cm on the
left side in our study. The previous study
reported mean circumference diameter of the distal
radius was which were 8.40 ± 0.81 cm on the right
side and 8.38 ± 0.79 cm on the left side [2]. The
comparison of circumferential diameter of lower
end of radius showed right side diameter was
larger than the left side diameter its
statistically significant p value (Table 3). The
circumference diameter of the distal end of radius
fractures are frequently articular injuries,
resulting in disruption of both the radiocarpal
and distal radioulnar joints. Even though these
fractures may heal, there is a high incidence of
malunion, joint disability, and instability. This
emphasizes the importance of alignment correction,
preservation of normal radial length, and
reconstruction of the congruity of the radiocarpal
and radioulnar joints [25].The smooth carpal
articular surface is divided by a ridge into
medial and lateral areas, with the medial area
being quadrangular in shape and the lateral area
being triangular [1].
|
Table 3: Circumferential Diameter
of Distal end of the Radius – Left and
Right (Paired Sample t’ Test)
|
|
Paired Differences
|
T
|
df
|
Sig. (2-tailed)
|
|
Mean
|
Std. Deviation
|
Std. Error Mean
|
95% Confidence Interval of the Difference
|
|
Lower
|
Upper
|
|
.22766
|
1.04230
|
.15204
|
.53369
|
.07837
|
1.497
|
46
|
0.141
|
This indicates that
on the right bone, the predominant shape of the
medial facets was quadrangular, while the lateral
facets were mostly triangular. On the left side,
the lateral facets were predominantly triangular
and the medial facets were primarily quadrangular
(fig: 3). Previous study stated that shape of the
scaphoid facet was found to be triangular, and the
lunate facet was quadrilateral in Indian study
[20]. There is limited information available in
the literature regarding the shapes of the facet.
However, the structure of the scaphoid and lunate
facet is crucial for diagnosing, treating
fractures and dislocations, as well as identifying
and correcting deformities such as Madelung
deformity. To the best of our knowledge, details
regarding the shapes of the facets on the right
and left sides have not been documented in
previous studies.
The tendon injuries,
including both flexor and extensor tendons, are
associated with volar plating of distal radius
fractures [26]. Although tendon damage is
influenced by the surgeon's skill and technique,
improper measurements or anatomical variations can
also alter the outcome.
Morphometric values
of the distal end of the radius vary among
different races, yet orthopaedic surgeons follow
fracture treatment protocols and reference values
based on western population, which may not be
suitable for the Indian population [20] due to
genetic variations, diet and nutrition that
affects the bone mass and density. The restoration
of normal range of motion, grip strength, and pain
relief, as well as the prevention of
post-traumatic arthritis caused by misalignment
and complications such as tendon or nerve damage,
all depend on proper alignment of fractures with
accurate measurements of the lower end of the
radius and the correct articular shape and
surface.
Conclusions
This study aimed to analyze the measurements and
shape variations of the distal end of the radius.
In the present study data findings guiding as a
reference for orthopedic surgeons and
radiologist’s essential aiding in prosthetic and
reconstructive surgeries and enhancing clinical
outcomes.
Acknowledgements
The authors sincerely wish to thank the
management, administrators and the Professor and
Head of the department of Anatomy of Vinayaka
Mission’s Kirupananda Variyar Medical College and
Hospitals, Salem for their whole hearted support
and permission to utilize the resources and
conduct this study. The authors acknowledge the
great help received from the scholars whose
articles are cited and included in references of
this manuscript. The authors are also grateful to
authors, editors and publishers of all those
articles, journals and books from where the
literature for this article has been reviewed and
discussed.
References
- Standring S. Gray’s Anatomy. Anatomical basis
of clinical practice, Churchill Livingstone,
40th ed, London. 2008; p 840-841.
- Rayna BS, Francis YM, Baskaran SB, Gouthaman
P, Begum Z. Morphometric Study of Proximal and
Distal End of Radius and its Clinical
Significance. J. Clin. Diagn. 2018;12(9):
AC09-AC12.
- Rennie L, Court-Brown CM, Mok JY, Beattie TF .
The epidemiology of fractures in children. J.
of. Injury. 2007; 38: 913–922.
- Rauch F, Neu C, Manz F, Schoenau E. The
development of metaphyseal cortex–implications
for distal radius fractures during growth. J
Bone Miner Res. 2001; 16(8): 1547–55.
- Baron JA, Karagas M, Barrett J, et al . Basic
epidemiology of fractures of the upper and lower
limb among Americans over 65 years of age. J.
Epidemiol. 1996; 7: 612–618.
- Gasse N, Lepage D, Pem R et al . Anatomical
and radiological study applied to distal radius
surgery. Surg. Radiol. Anat. 2011;
33(6): 485–490.
- Omsland TK, Ahmed LA, Gronskag A, et al. More
forearm fractures among urban than rural women:
the NOREPOS study based on the Tromso study and
the HUNT study. J. Bone Miner. Res.
2011;26: 850–856
- Meena S, Sharma P, Sambharia AK, Dawer A.
Fractures of Distal Radius: An Overview. J
Family Med Prim Care. 2014; 3(4): 325-332.
- Natarajan MV, Bose JC, Viswanath J,
Balasubramanian N, Sameer M. Custom prosthetic
replacement for distal radial tumours. Int.
Orthop. 2009; 33(4): 1081–1084.
- Leung F, Ozkan M, Chow SP. Conservative
treatment of intra articular fractures of the
distal radius and factors affecting functional
outcome. Hand Surg. Am. 2000;
5(2): 145-153.
- Slutsky DJ. Predicting the outcome of distal
radius fractures. Hand Clin. 2005; 21
(3): 289-94.
- Kulkarni RS, Kulkarni RA, Kulkarni RR,
Deshpande RS, Kulkarni SR. Long term trends in
the incidence of distal radius fractures in
Sindhudurg, west coast of Maharashtra
Retrospective analysis of 1776 distal radius
fractures Hospital based study. Indian J
Orthop Surg. 2024; 10(1): 48–54.
- Oppermann J, Wacker M, Stein G et al.
Anatomical fit of seven different palmar distal
radius plates. Arch. Orthop. Trauma Surg. 2014;
134(10):1483–1489.
- Kwak DS, Lee JY, Im JH, Song HJ, Park D. Do
volar locking plates fit the volar cortex of the
distal radius?. J. Hand Surg. Eur. 2017;
42 (3): 266–270.
- Werner FW, Palmer AK, Fortino MD, Short WH.
Force transmission through the distal ulna:
effect of ulnar variance, lunate fossa
angulation, and radial and palmar tilt of the
distal radius. J Hand Surg Am. 1992;
17(3): 423- 428.
- Johnson PG, Szabo RM. Angle measurements of
the distal radius: A cadaveric study. Skeletal
Radiol. 1993; 22(4): 243- 246.
- Evans S, Ramasamy A, Deshmukh SC. Distal volar
radial plates: how anatomical are they?
Orthopaedics and Traumatology. Int. J. Surg.
Res. Pract. 2014; 100(3): 293–295
- Standring S, Gray H. Gray’s anatomy the
anatomical basis of clinical practice. 41st ed,
Borley NR, Philadelphia, Elsevier Limited. 2016;
p 839- 840.
- Pogue DJ, Vegas SF, Patterson RM, Peterson PD,
Jenkins DK, Sweo TD, et al . Effects of distal
radius malunion on wrist joint mechanics. J.
Hand Surg. Am. 1990; 15:721‑727.
- Singh A, Saxena P, Gupta R, Singh A.
Morphometric Analysis of Distal End of Dry Human
Radius in Northern India and Its Clinical
Implications in Relation to Wrist Joint and
Inferior Radioulnar Joint Arthroplasty: A
Cross-sectional Study. Int. J. Anat. Radiol.
Surg. 2024; 13(2): AO01-AO07.
- Bruckner JD, Alexander AH, Lichtman DM. Acute
dislocations of the distal radioulnar joint. Instr.
Course Lect. 1996; 45: 27-36
- Kadel M, Thapa TP. Morphometric study of
distal end of human dry radii. Med. J. Shree
Birendra Hosp. 2021;
20(1):36- 40.
- Mittal A, Goyal GL, Mittal A. Morphometry of
distal end radius-surgical implication in
colles’ fracture. J. Evol. Med. Dent. Sci. 2019;
8 (42): 3100-3104.
- Gupta C, Kalthur SG, Malsawmzuali JC, D’Souza
AS. A morphological and morphometric study of
proximal and distal ends of dry radii with its
clinical implications. Biomed. J. 2015;
38 (4): 323-328.
- Suman NV, Chincholi S. Study of occurrence of
fracture of distal radius in Indian adult
population. Int. J. Orthop. Sci. 2020;
6(1): 50-52.
- Monaco NA, Dwyer CL, Ferikes AJ, Lubahn JD.
Reporting of Tendon Rupture Following Distal
Radius Volar Plating. J. Hand Surg. Am. 2016
;11(3): 278-286.
|




