|
Introduction
Ensuring
public access to quality healthcare services
relies on the fair distribution of health
resources such as healthcare professionals across
different geographical areas. The distribution of
health resources in a specific geographical area
greatly impacts people's access to healthcare [1].
Shreds of evidence indicate that a higher density
of healthcare professionals has a positive
correlation with health outcomes [2-3], healthcare
accessibility [4-6], and healthcare utilization
[7]. This underlines the significance of policies
that aim at increasing the supply of healthcare
professionals to improve health outcomes,
healthcare utilization, and healthcare equity.
Globally, ensuring fairness in distributing
healthcare resources is considered a major
challenge in the healthcare sector [8]. The
allocation of healthcare resources in countries
can be influenced by political factors that
frequently dictate resource allocation,
disregarding the populations' health needs in a
specific area [9]. The knowledge of the
distribution of healthcare professionals helps
determine if the distribution of the healthcare
professionals aligns with the population's health
needs. This will shed light on broader health
system challenges such as variations in the
quality of healthcare, disparities in healthcare
access, and informing strategies to improve health
services [10-16].
Health services in
the Kingdom of Saudi Arabia (KSA) have
significantly improved in the last two decades,
with greater access to healthcare resources
nationwide. The Ministry of Health (MOH) is the
major provider with about 60% of all services, and
the remaining share is divided among other
government and private sectors [17-18]. Since the
early 1990s, the private sector, the main provider
of health services for expatriate workers played a
role in the enhancements of healthcare delivery
through employer-contributed health insurance.
With the improved health services, there has been
a substantial increase in the number of healthcare
professionals over the last few years. According
to the MOH’s statistical yearbook, there were
105,332 physicians, 23897 dentists, 200,558 nurses
and midwives, and 34,040 pharmacists in the
Kingdom in 2022 [19]. Between 2010 and 2022, the
Kingdom recorded a 95.8% increase in physicians
(including dentists), 54.5% in nurses and
midwives, and 128% in pharmacists. Even though the
ratio of physicians, nurses, and pharmacists per
10,000 people increased in 2022, it is still lower
than in other high-income countries [20].
Currently, the ratio of physicians per 10,000
people in the KSA (31) is lower compared to
Germany (45), the USA (36), the UK (32), and the
European Union (43). The number of 56 nurses and
midwives per 10,000 people in the KSA is much
lower compared to Germany (123), the USA (125),
the UK (92), and the average for the European
Union (77) [20]. However, the number of
pharmacists in the KSA (9.35 pharmacists per
10,000 people) is comparable with countries such
as the UK (9.06), the USA (9.6), and Australia
(9.3). [20]. In comparison to other Gulf
Cooperation Council (GCC) countries, the KSA has a
higher physician-to-population ratio, whereas
Qatar (72) and the United Arab Emirates (64) have
higher nurse-to-population ratios [20].
Saudi Vision 2030
aims to transform the healthcare system in Saudi
Arabia, with a significant focus on improving the
distribution and composition of healthcare
professionals [21]. The National Transformation
Program (NTP) 2020 places a strong emphasis on
achieving equal distribution of health resources
across all regions of the Kingdom [22]. The aim is
to create a more equitable healthcare system that
provides high-quality services to all citizens and
expatriates, regardless of their location within
the Kingdom. This approach aligns with the broader
goals of Saudi vision-2030 to improve the
population’s health and well-being [23]. Moreover,
the Saudi health system is significantly affected
by the rising number of non-communicable diseases
(NCDs) and the increasing aging population,
specifically concerning the distribution of
healthcare resources [24-25]. Additionally,
chronic illnesses such as heart diseases, cancers,
and diabetes, are becoming more prevalent due to
changing lifestyles and aging, leading to a
greater need for prolonged medical treatment and
subsequently higher demand for healthcare
professionals [24].
The need for
healthcare services and hence healthcare
professional requirements across regions vary
depending on morbidity and mortality patterns.
Moreover, the composition of morbidity and
mortality may differ by region. The regions with
lower population density may require a greater
health professionals-population ratio [13].
Therefore, achieving a balanced and equitable
distribution of healthcare resources according to
demographic and geographical aspects is a real
challenge in most countries [26]. Recent studies
conducted in various countries used techniques
like Gini coefficients and Theil index for
assessing the geographical inequalities in the
distribution of health resources including the
health workforce. A study in Iran used Gini
coefficient and Hirschman-Herfindahl index to
assess fairness in the distribution of healthcare
specialists [27]. Recent studies in China employed
the Gini coefficients and Theil index to assess
the geographical inequalities in the distribution
of health resources [28-30]. In the KSA, existing
studies show that resources are distributed fairly
at the national level, but there are noticeable
differences in the distribution of physicians,
nurses, and pharmacists between regions, with
urban areas typically having better access than
rural areas [17, 24]. Few studies conducted in the
KSA showed disparities in terms of healthcare
access, and resources. For instance, a study in
Riyadh showed that a significant proportion of the
population had to travel long distances to access
healthcare services [26]. A study by Hawsami and
Abouammoh (2022) highlighted inequalities in the
distribution of hospital beds in the private
sector [31]. Similarly, a study on the
distribution of primary healthcare centers in the
KSA highlighted a significant regional disparity
across various health regions [32]. However,
another study by Kattan and Alshareef (2022)
showed a relatively equitable distribution of
hospital beds across various regions [33]. This
study addresses a critical gap in the literature
by measuring inequalities in the distribution of
health professionals across health regions of the
KSA using the Gini coefficients and Lorenz Curves.
While other studies have used Gini coefficients
and Lorenz curves to measure healthcare inequality
globally, this research applies these metrics to
the unique healthcare landscape of the KSA,
offering country-specific insights. Moreover, in
the KSA no attempt has ever been made to assess
the current status of the distribution of
healthcare professionals across different health
regions.
Therefore, this
research addresses the research question “to what
extent do the 20 health regions in the KSA differ
in their availability and density of healthcare
professionals’. The research assesses the equity
in the distribution of healthcare professionals in
the health regions based on the recent data
published by the MOH. The study pinpoints the
deficiencies in the distribution of healthcare
professionals and identifies the health regions
that are not keeping pace with the overall
development of healthcare professionals in the
Kingdom. It also provides an estimate of
additional requirements for healthcare
professionals in regions based on global
standards. The specific benchmark threshold levels
for physicians, dentists, nurses, and pharmacists
to achieve the universal health coverage (UHC)
effective coverage index based on the Global
Burden of Disease Study 2019 was used. By
addressing these gaps, the study contributes
valuable country-specific data to inform targeted
interventions and policies aimed at improving
health equity in the KSA. It is also expected that
the findings of the study could aid in
implementing necessary policy interventions and
promoting discourse on healthcare equity and
resource allocation in the KSA.
Materials and Methods
Study design and setting
In this research, a
secondary data analysis was conducted to assess
the distribution of physicians, dentists, nurses
and midwives, and pharmacists across the 20 health
regions of the KSA in 2022. Data on the number of
physicians, dentists, nurses (including midwives),
pharmacists employed by the MOH and the private
sector, and demographic information for each
region were obtained from the statistical Yearbook
of the MOH, which is viewed as an authentic source
of information on health-related data in the KSA.
The MOH statical yearbook provides detailed
information on healthcare professionals of all
regions in the KSA as reported to the Ministry at
the end of each year. This study includes data on
MOH facilities and private health facilities
across 20 health regions. The analysis considered
the population of both Saudi citizens and
expatriates, across the health regions. The
estimates of the population for 2022 in the
regions were compiled from the MOH Statistical
Yearbook [19]. This is the mid-year population
estimate produced by the national statistical
agencies. In this research population estimate for
2022 was used to estimate the density of
healthcare professionals per 10,000 population in
20 regions [19]. This measure is regarded as a
standardized unit of measurement for comparing the
availability of healthcare professionals across
different regions with varying population sizes
[28]. It would also serve as a measure of the
healthcare services access in different regions in
the KSA.
Study tools
and data extraction
A spreadsheet was
created using Microsoft Excel 2016 to retrieve
data such as health region, year, population,
physicians, nurses, and pharmacists from the MOH
Statistical Yearbook. To evaluate the equity in
the allocation of healthcare professionals such as
physicians, dentists, nurses, and pharmacists
across 20 health regions, the Lorenz curve and
Gini coefficient were computed and visualized with
Excel, 2016. While the Lorenz curve is a graphical
tool that allows for comparing inequalities about
a state of perfect equality, the Gini coefficient
is a statistical measure utilized to evaluate
disparities in the distribution of resources in
society [34]. The Gini coefficient is the most
commonly used measure of inequality, making it
easily understood and comparable across different
studies and contexts. The Gini coefficient is
independent of the size of the economy and the
size of the population, making it suitable for
comparing regions with different population sizes.
This measure is more sensitive to changes around
the middle of the distribution than at the very
top and bottom, which can be useful for capturing
changes in the distribution of health
professionals [35].
In the Lorenz curve,
the x-axis shows the cumulative percentage of the
population, the y-axis depicts the total
percentage of healthcare professionals in the
regions. The graph displays a diagonal line to
represent perfect equality, with the Lorenz curve
typically situated beneath it. The Gini
coefficient is computed from the graph by
comparing the area below the diagonal line with
the curve to the total area under the line of
equality [34]. The interpretation of the different
Gini coefficient values is presented in Table 1.
|
Table 1: Interpretation of the Gini
coefficient values
|
|
Gini coefficient
|
Evaluation of equity
|
|
≤ 0.2
|
Perfect equality
|
|
> 0.2–0.3
|
Relative equality
|
|
> 0.3–0.4
|
Adequate equality
|
|
> 0.4–0.5
|
Large equality gap
|
|
> 0.5
|
Severe equality gap
|
In this research,
additional requirements for physicians, dentists,
nurses, and pharmacists in regions were estimated
based on a threshold level established based on
the Global Burden of Disease Study 2019. For the
first time, Haakenstadsed et al (2022) calculated
healthcare professionals thresholds for
physicians, dentists, nurses and midwives, and
pharmacists using the universal health coverage
(UHC) effective coverage index [36]. These
thresholds are essential to reach target UHC
levels if countries efficiently utilize the
healthcare professionals for UHC. To achieve a
score of 80 on the UHC effective coverage index,
for every 10,000 people, a minimum of 20.7
physicians, 8.2 dentists, 70.6 nurses and
midwives, and 9.4 pharmaceutical personnel would
be required.
Results
Table 2 shows the
overall availability of physicians, dentists,
nurses and midwives, and pharmacists in The KSA
during the last five years (2018-2022). The
country, which houses about 32.2 million people,
has 32.74 physicians, 7.43 dentists, 62.33 nurses
and midwives, and 10.58 pharmacists per 10,0000
people in 2022. This number only reflects the
overall healthcare professionals capacity in the
Kingdom, but hides significant regional
differences in the distribution of various
categories of health professionals.
|
Table 2: Five-year availability of
healthcare professionals in the KSA from
2018 to 2022*
|
|
Year
|
Population
|
Category
|
Number
|
Per 10,000 people
|
|
2018
|
29,647,968
|
Physicians
|
88023
|
29.68
|
|
Dentists
|
16752
|
5.65
|
|
Nurses and Midwives
|
184565
|
62.25
|
|
Pharmacists
|
29125
|
9.82
|
|
2019
|
30,196,281
|
Physicians
|
94335
|
31.24
|
|
Dentists
|
18811
|
6.23
|
|
Nurses and Midwives
|
199013
|
65.90
|
|
Pharmacists
|
31872
|
10.55
|
|
2020
|
30,063,799
|
Physicians
|
95336
|
31.71
|
|
Dentists
|
19622
|
6.53
|
|
Nurses and Midwives
|
196701
|
65.43
|
|
Pharmacists
|
27529
|
9.16
|
|
2021
|
31,552,510
|
Physicians
|
99617
|
38.78
|
|
Dentists
|
22739
|
7.21
|
|
Nurses and Midwives
|
201489
|
63.85
|
|
Pharmacists
|
30840
|
9.77
|
|
2022
|
32,175,224
|
Physicians
|
105332
|
32.74
|
|
Dentists
|
23897
|
7.43
|
|
Nurses and Midwives
|
200558
|
62.33
|
|
Pharmacists
|
34040
|
10.58
|
Source: Compiled
from the Annual Statistical Yearbook, MOH,
KSA,2022
Note: * This data
includes physicians, dentists, nurses and
midwives, and pharmacists employed in the MOH
health facilities, other government
ministries/agencies, and the private sector
Table 3 provides
region-wise distribution of physicians, dentists,
nurses and midwives, and pharmacists employed in
the facilities owned and managed by the MOH and
the private health sector in 2022.
|
Table 3: Healthcare professionals
employed in health regions of the KSA,
2022
|
|
Health Region
|
Physicians
|
Number of Dentists
|
Nurses and midwives
|
Pharmacists
|
|
Taif
|
3184
|
731
|
5919
|
952
|
|
Jeddah
|
10940
|
2942
|
15965
|
4473
|
|
Makkah
|
5551
|
1219
|
8263
|
1772
|
|
Riyadh
|
20385
|
6279
|
38442
|
10995
|
|
Al-Ahsa
|
3197
|
720
|
6754
|
770
|
|
Eastern
|
9627
|
2248
|
19302
|
2866
|
|
Qaseem
|
4275
|
1112
|
8692
|
1544
|
|
Madina
|
5527
|
1418
|
10892
|
1571
|
|
Tabouk
|
2340
|
553
|
4511
|
802
|
|
Bishah
|
1154
|
259
|
1957
|
245
|
|
Aseer
|
4591
|
1307
|
8251
|
1639
|
|
Hafr Al Baten
|
1136
|
331
|
3528
|
315
|
|
Najran
|
1740
|
377
|
3620
|
409
|
|
Jazan
|
3440
|
729
|
6863
|
1169
|
|
Northern
|
1509
|
253
|
3177
|
339
|
|
Hail
|
2269
|
575
|
4541
|
697
|
|
Qunfudah
|
789
|
161
|
1138
|
175
|
|
Qurayyat
|
512
|
146
|
1958
|
123
|
|
Al-Jouf
|
1486
|
280
|
3830
|
314
|
|
Al Baha
|
1588
|
318
|
2354
|
239
|
|
Total
|
85240
|
21958
|
159957
|
31409
|
Source: Compiled from the Annual Statistical
Yearbook, MOH, KSA,2022.
(Data relates to health professionals employed by
the MOH and private sector)
A thorough
examination of the distribution of healthcare
professionals 10000 people in 20 health regions in
the KSA provides valuable information about the
healthcare system (Table 4).
|
Table 4: Physicians, Dentists, Nurses,
and Pharmacists per 10,000 population in
Health Regions
|
|
Region
|
Population
|
Physicians
|
Dentists
|
Nurses and Midwives
|
Pharmacists
|
|
Taif
|
1101571
|
28.90
|
6.63
|
53.73
|
8.64
|
|
Jeddah
|
3971816
|
27.54
|
7.41
|
40.19
|
11.26
|
|
Makkah
|
2677810
|
20.72
|
4.55
|
30.85
|
6.62
|
|
Riyadh
|
8591748
|
23.73
|
7.31
|
44.74
|
12.79
|
|
Al-Ahsa
|
1104267
|
28.95
|
6.52
|
61.16
|
6.97
|
|
Eastern
|
3553980
|
27.08
|
6.32
|
54.31
|
8.06
|
|
Qaseem
|
1336179
|
31.99
|
8.32
|
65.05
|
11.55
|
|
Madina
|
2137983
|
25.85
|
6.63
|
50.94
|
7.34
|
|
Tabouk
|
886036
|
26.41
|
6.24
|
50.91
|
9.05
|
|
Bishah
|
309528
|
37.28
|
8.36
|
63.22
|
7.92
|
|
Aseer
|
1714757
|
26.77
|
7.62
|
48.11
|
9.56
|
|
Hafr Al Baten
|
467007
|
24.32
|
7.08
|
75.54
|
6.74
|
|
Najran
|
592300
|
29.37
|
6.36
|
61.11
|
6.91
|
|
Jazan
|
1404997
|
24.48
|
5.18
|
48.84
|
8.32
|
|
Northern
|
373577
|
40.39
|
6.77
|
85.04
|
9.07
|
|
Hail
|
746406
|
30.39
|
7.70
|
60.83
|
9.33
|
|
Qunfudah
|
270266
|
29.19
|
5.95
|
42.11
|
6.47
|
|
Qurayyat
|
195016
|
26.25
|
7.48
|
100.40
|
6.31
|
|
Al-Jouf
|
400806
|
37.07
|
6.98
|
95.55
|
7.83
|
|
Al Baha
|
339174
|
46.82
|
9.37
|
69.40
|
7.04
|
|
Total
|
32175224
|
26.49
|
6.82
|
49.71
|
9.76
|
Source: Calculated by the authors based on MOH
data (Data relates to health professionals
employed by the MOH and private sector)
A comparison between
ratios of regional and national healthcare
professionals highlights significant disparities.
When it comes to regional distribution, 7 health
regions have a physician population ratio below
the national average, 9 regions have dentists
below the national level, and 4 regions have
nurses and midwives population ratio below the
national average, and 14 health regions have a
pharmacists-population ratio below the national
average. Health regions such as Riyadh, Makkah,
and Madina, have low physician-population ratios
compared to other regions, whereas regions like
Bishah, Northern, Al-Baha, and Al-Jouf show the
highest ratios at the opposite end of the
spectrum. This is in sharp contrast to the
country's average, showing a notable lack of
physicians, dentists, nurses, midwives, and
pharmacists in some regions. Further investigation
is needed on the distribution and accessibility of
resources for each population and their impact on
the effectiveness of delivering healthcare
services. The policymakers need to carefully
consider the empirical data to achieve the goals
of Saudi Vision 2030 and meet the needs of the
expanding Saudi population.
Equity in the distribution of healthcare
professionals
The distribution of
physicians in different regions of the KSA is even
as shown by Gini coefficient of 0.11. Fig 1 shows
the Lorenz curve, demonstrating the distribution
plotting the cumulative share of physicians
against the cumulative share of regions. The
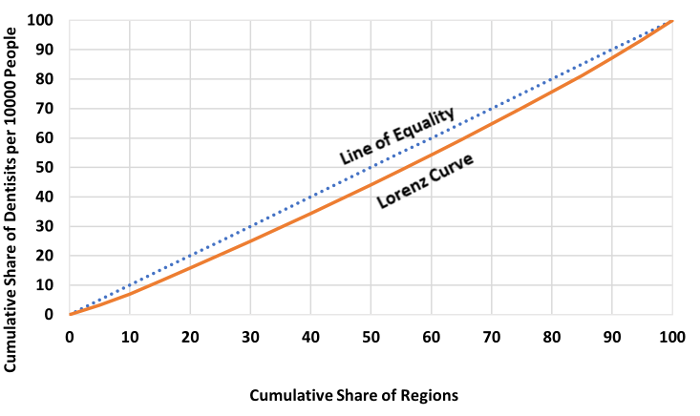
distribution of dentists in health regions shows a
Gini coefficient of 0.08 denotes an even
distribution of dentists across different regions
(Fig:2). The shape of the curve to the line of
equality indicates a perfect equality in the
distribution of dentists across all health
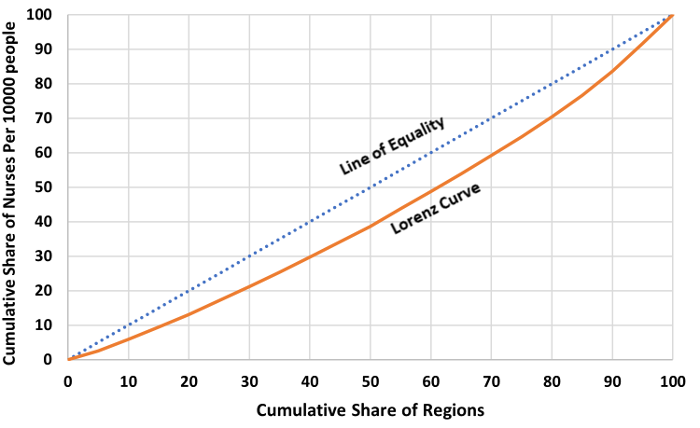
regions. The Gini coefficient of nurses and
midwives of 0.16 is slightly higher than
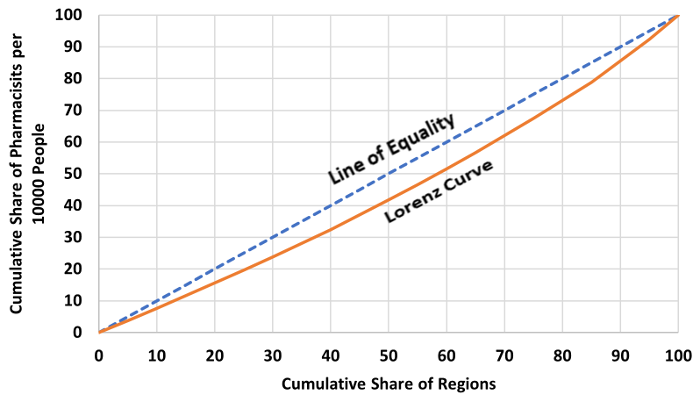
physicians and dentists (Fig 3). Similarly, the
Gini coefficient for pharmacists is 0.12, showing
an even distribution across the regions. These
Gini coefficients suggest a fair distribution of
physicians, nurses, and pharmacists across
regions, ensuring reasonably fair healthcare
access nationwide.
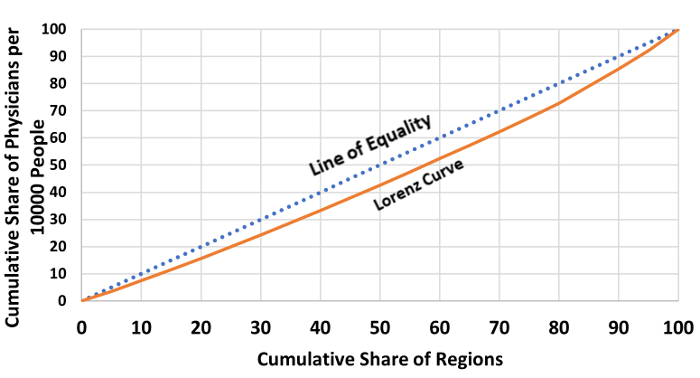
|
| Figure
1: Lorenz Curve showing the distribution
of physicians per 10,000 people in KSA
|
|
| Figure 2: Lorenz Curve
showing the distribution of dentists per
10,000 people in KSA |
|
| Figure 3: Lorenz Curve
showing the distribution of nurses and
midwives per 10,000 people |
|
| Figure 4: Lorenz Curve
showing the distribution of pharmacists
per 10,000 people |
Projection on the Enhancement in
Healthcare Professionals Distribution
An analysis was
conducted to assess healthcare professionals'
density across health regions in the KSA compared
to the global threshold level [36 ] aiming for a
minimum of 20.7 physicians, 8.2 dentists, 70.6
nurses and midwives, and 9.4 pharmacists per 10000
people to achieve the UHC index of 80 out of 100.
The analysis shows that all 20 health regions have
achieved the threshold level of physicians.
However, except for 2 regions namely Qaseem, and
Al Baha all regions registered a shortfall of
dentists below the threshold level. While 16
health regions have nurses and midwives below the
threshold level of 70.6 nurses and midwives per
10000 people; 15 regions have pharmacists fall
short of the threshold level of 9.4 pharmacists
per 10,000 people. Table 5 shows the current gaps
in distribution by region and the additional
number of dentists, nurses (including midwives),
and pharmacists required for each region to reach
the threshold level to achieve the UHC index of 80
out of 100. Figure 5 shows the shortage of health
professionals by administrative regions of the
KSA.
|
Table 5: Dentists, nurses, and
pharmacists needed to achieve the
threshold level
|
|
Health regions
|
Dentists needed to achieve a threshold
level (8.2 per 10,000 people)
|
Nurses and midwives needed to achieve a
threshold level (70.6 per 10,000 people)
|
Pharmacists needed to achieve a threshold
level of (70.6 per 10,000 people)
|
|
Required
|
Shortage
|
Percent
|
Required
|
Shortage
|
Percent
|
Required
|
Shortage
|
Percent
|
|
Taif
|
903
|
172
|
19.04
|
7777
|
1858
|
23.89
|
1035
|
84
|
8.11
|
|
Jeddah
|
3256
|
315
|
9.67
|
28041
|
12076
|
43.06
|
3733
|
+
|
+
|
|
Makkah
|
2196
|
977
|
44.48
|
18905
|
10642
|
56.29
|
2517
|
745
|
29.60
|
|
Riyadh
|
7045
|
766
|
10.87
|
60657
|
22216
|
36.62
|
8076
|
+
|
+
|
|
Al-Ahsa
|
905
|
186
|
20.55
|
7796
|
1042
|
13.36
|
1038
|
268
|
25.81
|
|
Eastern
|
2914
|
666
|
22.85
|
25091
|
5789
|
23.07
|
3341
|
475
|
14.22
|
|
Qaseem
|
1096
|
+
|
+
|
9433
|
+
|
+
|
1256
|
+
|
+
|
|
Madina
|
1753
|
335
|
19.11
|
15094
|
4202
|
27.83
|
2010
|
439
|
21.84
|
|
Tabouk
|
727
|
174
|
23.93
|
6255
|
1744
|
27.88
|
833
|
31
|
3.72
|
|
Bishah
|
253
|
5
|
1.97
|
2185
|
228
|
10.43
|
291
|
46
|
15.80
|
|
Aseer
|
1406
|
99
|
7.04
|
12106
|
3855
|
31.84
|
1612
|
+
|
+
|
|
Hafr Al Baten
|
383
|
52
|
13.57
|
3297
|
+
|
+
|
439
|
124
|
28.24
|
|
Najran
|
486
|
109
|
22.42
|
4183
|
562
|
13.43
|
557
|
148
|
26.57
|
|
Jazan
|
1152
|
423
|
36.71
|
9919
|
3056
|
30.80
|
1321
|
152
|
11.50
|
|
Northern
|
306
|
53
|
17.32
|
2637
|
+
|
+
|
351
|
12
|
3.41
|
|
Hail
|
612
|
37
|
6.04
|
5270
|
729
|
13.83
|
701
|
5
|
0.71
|
|
Qunfudah
|
221
|
61
|
27.60
|
1908
|
770
|
40.35
|
254
|
79
|
31.10
|
|
Qurayyat
|
159
|
14
|
8.80
|
1376
|
+
|
+
|
183
|
60
|
32.78
|
|
Al-Jouf
|
328
|
49
|
14.93
|
2830
|
+
|
+
|
377
|
63
|
16.71
|
|
Al Baha
|
278
|
+
|
+
|
2394
|
41
|
1.71
|
319
|
80
|
25.07
|
|
Total
|
26379
|
4483
|
|
227154
|
68810
|
|
30244
|
2811
|
|
Note: + refers to not required
or excess.

|
| Figure
5: Administrative regions with shortage of
healthcare professionals |
The research
highlighted the additional requirements for 4493
dentists, 69551 nurses and midwives, and 2811
pharmacists to adhere to the global threshold
level of 8.2 dentists, 70.6 nurses and midwives,
and 9.4 pharmacists per 10000 population in
different regions to reach the UHC index of 80.
Discussion
To the best of our
understanding, this is the initial research that
assesses the equity in the distribution of
healthcare professionals based on population size
among different health regions in the KSA in 2022.
From the analysis and results of the Gini
coefficient, it appears the distribution of
physicians, dentists, nurses, and pharmacists is
equitable across various regions in the KSA. The
Gini coefficients obtained for physicians,
dentists, nurses, and pharmacists are 0.11, 0.08,
0.16, and 0.12 respectively. Nevertheless, a stark
contrast in terms of healthcare professionals is
apparent when analyzing the 20 health regions in
comparison to the national averages of doctors,
dentists, nurses, and pharmacists. Roughly 65% of
the regions have physicians below the national
average, whereas 50% of regions have dentists
below the national level. While 30% of regions
have nurses and midwives below the national level,
a majority of the health regions (85%) have
pharmacists below the national average.
Notably, regions
such as Riyadh, Makkah, and Madina exhibit
significantly lower physician population ratios in
contrast to regions such as Bishah, Northern, and
Al Baha. This underscores the geographical
inequalities in the distribution of physicians.
The distribution of dentists across regions
reveals regions like Qaseem, Bishah, and Al Baha
have a higher number of dentists per 10,000
people, in contrast to regions like Mecca, Jazan,
and Qunfudah. While regions like Jeddah, Makkah,
Riyadh, and Qunfudah have a lower nurse and
midwives population ratio compared to the national
average, Qurayyat and Al-Jouf regions have nurses
and midwives double the national average. This
highlights the uneven distribution of healthcare
professionals across different geographical
regions in the KSA.
The study also
highlighted those significant economic regions
such as Makkah, Jeddah, Riyadh, and Madina showed
a lower healthcare professionals population ratio
compared to other regions. Makkah region, the
Holiest place for Muslims attract millions of
pilgrims and surge in visitors put enormous
pressure on healthcare system in the region [37].
It should also be noted that this region recorded
the high prevalence of COVID-19 cases in 2020,
constituting 49.3% of all cases in the Kingdom.
Makkah region faced inadequate availability of
healthcare resources including physicians, and ICU
hospital beds during the pandemic [38]. Therefore,
enhancing the availability of healthcare resources
including healthcare professionals distribution in
this region should be given higher priority.
Similarly, the study
showed that health regions such as Jeddah and
Riyadh have a low ratio of physicians, dentists,
nurses and pharmacists, highlighting a notable
shortage of the health professionals. Several
factors like population growth, increasing
economic activities, and urbanization in these
health regions pose challenges in effectively
providing access to healthcare services [31,39].
Despite their economic significance, these regions
lag in health professional distribution [32].While
specific numbers of health professionals employed
in the OGH sector in Riyadh and Jeddah are not
provided, it can be inferred that these cities may
have a better supply of health professionals
compared to other regions due to their urban
status.
Furthermore,
imbalanced allocation of healthcare resources such
as hospital beds, healthcare professionals and
primary healthcare centers could significantly
influence health outcomes. Earlier studies have
identified the issues of access to healthcare
services such as inadequate capacity of primary
healthcare centres, and hospital beds in Jeddah
region [38]. A rapid urbanization in Riyadh region
also poses challenges in equal distribution of
healthcare resources in all clusters [40].
Therefore, a more detailed comprehension of the
causes of disparities in health resources
distribution in densely populated areas like
Jeddah and Riyadh regions is needed.
The Gini
coefficients showed good indicator of equality in
the distribution of healthcare professionals among
the 20 health regions. The coefficients for
physicians, dentists, nurses and midwives, and
pharmacists falls under perfect equality, which
implies the health regions in the KSA have
relatively fair distribution of healthcare
professionals comparable to their population. The
proximity to the line of equality suggests minimal
disparity in the distribution of healthcare
professionals. Few studies have highlighted
disparities in the distribution of primary
healthcare centres, and hospital beds across
various regions in the KSA. Al Sheddi et al (2023)
estimated the Gini coefficient, which measures
inequality, indicated relative equality in primary
healthcare centre distribution across the 20
health regions, with values between 0.2 and 0.3.
The study found certain regions exhibited
disparities, suggesting the need for more
equitable distribution to improve healthcare
access and outcomes [41]. A study by Saffer et al
(2021) showed variations in the distribution of
primary healthcare centers across health regions,
and within regions, specialized healthcare
professionals are concentrated in urban areas
[42].
The disparities in
the distribution of health professionals have
significant practical implications for healthcare
delivery in underserved regions. These
implications manifest in various ways, affecting
both the quality and accessibility of healthcare
services. The shortage of health professionals in
the regions may cause longer wait times for
appointments, increased travel distances for
patients seeking care, reliance on emergency
services for non-urgent care, delayed diagnoses
and treatments, particularly in critical and
emergency cases. The shortage of health
professionals would also lead to overworked
healthcare providers, potentially leading to
burnout and reduced quality of care [43-45].
Studies have found the shortage of health
professionals may cause limited time for patient
consultations, affecting the thoroughness of
examinations and treatments, and insufficient
provision of preventive and primary care services
[45]. There are challenges in providing culturally
competent care, which is crucial for effective
healthcare delivery, and limited access to
specialists and advanced treatments in underserved
areas [44].
Authors have
estimated that additional requirements for 4493
dentists, 69551 nurses and midwives, and 2811
pharmacists to adhere to the global benchmark of
8.2 dentists, 70.6 nurses and midwives, and 9.4
pharmacists per 10000 people. This research has
also revealed that all health regions in the KSA
have achieved a threshold level of physicians of
20.7 per 10,000 people to achieve a UHC index of
80%. However, there are geographical inequalities,
particularly highly populated regions have lower
physician-population ratios compared to other
regions. The distribution of dentists across
health regions shows that Qaseem and Al Baha have
achieved a threshold level of 8.2 dentists per
10,000 people. With regard to the distribution of
nurses and midwives regions such as Hafr Al Baten,
Northern, Qurayyat, and Al Jouf have achieved a
threshold level of 70.6 nurses and midwives per
10,000 people. Regions like Jeddah, Makkah,
Riyadh, Qaseem, and Aseer have achieved a
threshold level of 9.4 pharmacists per 10,000
people.
Policy Implications
The study provides
several actionable insights that directly support
Saudi Vision 2030. It helps to identify potential
shortages or surpluses in health professionals in
the health regions. This information is crucial
for planning the healthcare workforce to meet the
changing needs of the population in health
regions. It also provides a roadmap for
policymakers to address future imbalances between
healthcare supply, and demand, directly supporting
the healthcare transformation goals of Saudi
Vision 2030. Future research incorporating GIS in
the spatial distribution of healthcare facilities
may provide a deeper understanding of
accessibility challenges. This data could be
extremely valuable for making precise policy
decisions and determining where to invest in new
healthcare infrastructure and improve access to
healthcare services. Future research should also
offer a foundation for a continuous dialogue and
investigation on methods to achieve a fairer
allocation of healthcare resources including
healthcare professionals in the KSA and create a
system that can adapt to the changing healthcare
needs of its people.
Study Limitations
Despite providing
valuable information on the distribution of
healthcare professionals in the KSA, this study
has certain limitations. The findings of this
study dependent on the accuracy and
comprehensiveness of the data from the MOH's
Statistical Yearbook 2022. Despite being a
reliable source, the MOH Yearbook may lack the
ability to accurately represent current changes or
the details of the health professionals. Moreover,
this research mainly focused on quantitative data,
neglecting qualitative insights into the reasons
behind workforce disparities. Qualitative data is
crucial for understanding the context and
underlying factors contributing to workforce
disparities. Secondary data often fails to account
for cultural and social factors that may influence
workforce disparities, such as gender roles or
regional differences in employment opportunities.
The Gini coefficient does not consider that
individuals may utilize health services in nearby
regions. This constraint is especially concerning
in areas with varying population densities, as it
could overestimate inequality in sparsely
populated regions.
Furthermore, the
focus of this research is restricted to 2022,
offering a snapshot rather than a longitudinal
view. Thus, the analysis does not consider the
trends in the distribution of healthcare
professionals over time or the effects of recent
reforms in the Saudi healthcare system. To address
these limitations, it would be beneficial to
complement the MOH data with qualitative studies
that explore the experiences and perspectives of
healthcare professionals, employers, and
policymakers. This approach would provide a more
comprehensive understanding of workforce
disparities and help inform more effective
policies and interventions in Saudi Arabia's
healthcare sector.
Conclusion
This research
highlights a critical component in the progress of
the KSA's healthcare system, characterized by the
challenge of balancing rapid economic development
with the equitable distribution of health
resources. The results showed notable differences
in health professionals’ availability in various
regions, especially in densely populated areas
such as Makkah, Riyadh, and Jeddah, underscoring
the shortfall in addressing the healthcare
requirements of the whole population. This
imbalance not only reflects the current state of
healthcare availability but also raises concerns
about the system's readiness to manage the growing
NCDs and the requirements of an aging population.
Therefore, addressing these inequalities will be
crucial for achieving Saudi Vision 2030 and
improving overall healthcare provision across the
country. Nonetheless, this research provides
valuable insights into the present status of
healthcare professionals' distribution in the KSA.
The existing inequalities amongst the health
regions can be reduced by introducing strategies
such as providing additional incentives,
increasing the retirement age in remote regions,
introducing bridge programs to upgrade the skills
of diploma-holding nurses, and expanding digital
health services. Additional strategies may include
investing in medical education, adopting policies
to increase the number of Saudi nationals in the
workforce, and implementing measures to improve
distribution across regions and between urban and
rural areas. These strategies collectively aim to
create a more equitable distribution of health
professionals across Saudi Arabia and improve
access to quality healthcare for all citizens
regardless of their location.
References
- Pan J, Shallcross D. Geographic distribution
of hospital beds throughout China: a
county-level econometric analysis. Int J
Equity Health 2016;15(1):179.
doi:10.1186/s12939-016-0467-9.
- Liu J, Eggleston K. The association between
health workforce and health outcomes: a
cross-country econometric study. Soc Indic
Res 2022;163(2):609-632.
- Basu S, Berkowitz S A, Phillips R L.
Association of primary care physician supply
with population mortality in the United States,
2005-2015. JAMA Intern. Med 2019;
179(4): 506–514.
- Wu Q, Wu L, Liang X, Xu J, Wu W, Xue Y.
Influencing factors of health resource
allocation and utilization before and after
COVID-19 based on RIF-I-OLS decomposition
method: a longitudinal retrospective study in
Guangdong Province, China. BMJ Open
2023;13(3):e065204.
- Ferretti F, Mariani M, Sarti E. Physician
density: will we ever close the gap? BMC Res
Notes 2023;16(1):84.
- Peters DH, Garg A, Bloom G, Walker DG, Brieger
W R, Rahman M H. Poverty and access to health
care in developing countries. Ann. N. Y.
Acad. Sci2008; 1136(1): 161–171.
- Leonard C, Stordeur S, Roberfroid D.
Association between physician density and health
care consumption: A systematic review of the
evidence. Health Policy.
2009;91(2):121-134.
- Omrani-Khoo H, Lotfi F, Safari H, Zargar
Balaye Jame S, Moghri J, Shafii M. Equity in
distribution of health care resources;
assessment of need and access, using three
practical indicators. Iran J Public Health.
2013;42(11):1299–308
- Mobaraki H, Hassani A, Kashkalani T,
Khalilnejad R, Chimeh EE. Equality in
distribution of human resources: the case of
Iran's ministry of health and medical education.
Iran J Public Health 2013;1:42.
- Sebai ZA, Milaat WA, Al-Zulaibani AA. Health
care services in Saudi Arabia: past, present and
future. J Family Community Med
2001;8(3):19–23.
- Rice N, Smith PC. Ethics and geographical
equity in health care. J Med Ethics
2001;27(4):256–61
- El-Farouk A. Geographical distribution of
health resources in the Kingdom of Saudi Arabia
: is it equitable? Egypt J Environ Change.
2016;8:4–20.
- Munga MA, Mæstad O. Measuring inequalities in
the distribution of health workers: the case of
Tanzania. Hum Resour Health 2009;7:4
(2009). Available at https://human-resources-health.biomedcentral.com/articles/10.1186/1478-4491-7-4.
- Nussbaum C, Massou E, Fisher R, Morciano M,
Harmer R, Ford J. Inequalities in the
distribution of the general practice workforce
in England: a practice-level longitudinal
analysis. BJGP Open.
2021;5(5):BJGPO.2021.0066. doi:
10.3399/BJGPO.2021.0066.
- Wang Y, Li Y, Qin S, Kong Y, Yu X, Guo K, Meng
J. The disequilibrium in the distribution of the
primary health workforce among eight economic
regions and between rural and urban areas in
China. Int J Equity Health 2020; 19:28 https://doi.org/10.1186/s12939-020-1139-3
- Wiseman V, Lagarde M, Batura N, Lin S, Irava
W, Roberts G. Measuring inequalities in the
distribution of the Fiji Health Workforce. Int
J Equity Health. 2017;16(1):115. doi:
10.1186/s12939-017-0575-1.
- Albejaidi F, Nair KS. Building the health
workforce: Saudi Arabia's challenges in
achieving Vision 2030. Int J Health Plann
Manage 2019;34(4):e1405-e1416. doi:
10.1002/hpm.2861
- Al-Hanawi MK, Khan SA, Al-Borie HM. Healthcare
human resource development in Saudi Arabia:
emerging challenges and opportunities—a critical
review. Public Health Rev 2019;40(1). https://doi.org/10.1186/s40985-019-0112-4.
- Ministry of Health, Statistical Yearbook.
Riyadh. Ministry of Health. 2022, Kingdom of
Saudi Arabia.
- World Health Organization. The Global Health
Observatory. https://www.who.int/data/gho.
- Kingdom of Saudi Arabia. Saudi Arabia's Vision
2030. http//www.vosion2030.gov.sa/en/ntp.
- Kingdom of Saudi Arabia. Saudi Arabia's
National Transformation Program.
https://vision2030.gov.sa / sites/default/
files/NTP_En.pdf.
- Alasiri AA, Mohammed V. Healthcare
transformation in Saudi Arabia: an overview
since the launch of Vision 2030. Health
Serv Insights 2022;3. doi: 10.1177/ 11786
329 2211 21 214.
- Albejaidi F, Nair K S. Nationalisation of
health workforce in Saudi Arabia’s public and
private sectors: a review of issues and
challenges. J Health Manag. 2021; 23(3).
Available at https://journals.sagepub.com/doi/abs/10.1177/09720634211035204
- Boettiger DC, Lin TK, Almansour M, Hamza MM,
Alsukait R, Herbst CH, et al.
Projected impact of population aging on
non-communicable disease burden and costs in the
Kingdom of Saudi Arabia, 2020–2030. BMC
Health Serv Res. 2023;23(1):1381.https://
doi. org/ 10. 1186/ s12913- 023- 10309-w.
- Mansour S. Spatial analysis of public health
facilities in Riyadh Governorate, Saudi Arabia:
a GIS-based study to assess geographic
variations of service provision and
accessibility. Geo Spatial Inform Sci.
2016;19(1):26–38.
- Nasiri A, Amerzadeh M, Yusefzadeh H, Moosavi
S, Kalhor R. Inequality in the distribution of
resources in the health sector before and after
the Health Transformation Plan in Qazvin, Iran.
J Health Popul Nutr 2024;43(1):4. doi:
10.1186/s41043-023-00495-y.
- Chen M, Chen X, Tan Y, Cao M, Zhao Z, Zheng W
et al. Unraveling the drivers of inequality in
primary health-care resource distribution:
Evidence from Guangzhou, China. Heliyon 2024;10(19):e37969.https://doi.org/10.1016/j.heliyon.2024.e37969
- Chai Y, Xian G, Kou R, Wang M, Liu Y, Fu G, et
al. Equity and trends in the allocation
of health human resources in China from 2012 to
2021. Arch Public Health 2024;82:175. https://doi.org/10.1186/s13690-024-01407-0
- Dong E, Sun X, Xu T, Zhang S, Wang T, Zhang L,
et al. Measuring the inequalities in
healthcare resource in facility and workforce: A
longitudinal study in China. Front. Public
Health. 2023;11:1074417. doi:
10.3389/fpubh.2023.1074417
- Hawsawi T, Abouammoh. Distribution of hospital
beds across Saudi Arabia from 2015 to 2019: a
cross-sectional study. EMHJ
2022;28(1):23-30.
- Kattan W. The state of primary healthcare
centers in Saudi Arabia: A regional analysis for
2022. PLoS One 2024; 19(9): e0301918. https://doi.org/10.1371/journal.pone.0301918.
- Kattan W, Alshareef N. 2022 Insights on
hospital bed distribution in Saudi Arabia:
evaluating needs to achieve global standards. BMC
Health Serv Res 2024;24(1):911. doi:
10.1186/s12913-024-11391-4.
- Bellu LG, Liberati P. Inequality analysis: The
Gini Index. 2005. Available at https://openknowledge.fao.org/server/api/core/bitstreams/a5e207ae-bff6-4a26-84b6-6108e318e706/content
- Joe Hasell. Measuring inequality: what is the
Gini coefficient? Published online at
OurWorldinData.org. Retrieved from:
'https://ourworldindata.org/what-is-the-gini-coefficient'
[Online Resource]. 2023.
- Haakenstad A, Irvine CMS, Knight M, Bintz C,
Aravkin AY, Zheng P, et al. Measuring
the availability of human resources for health
and its relationship to universal health
coverage for 204 countries and territories from
1990 to 2019: a systematic analysis for the
global burden of disease study 2019. Lancet
2022; 399: 2129–54.
- Alrefaei AF, Almaleki D, Alshehrei F, et al.
Assessment of health awareness and knowledge
toward SARS-CoV-2 and COVID-19 vaccines among
residents of Makkah. Saudi Arabia Clin
Epidemiol Glob Health. 2022;13:100935.
https:// doi. org/ 10. 1016/j. cegh. 2021.
100935.
- Arbaein TJ, Alharbi KK, Alfahmi AA, Alharthi
KO, Monshi SS, Alzahrani AM, et al.
Makkah healthcare cluster response, challenges,
and interventions during COVID-19 pandemic: a
qualitative study. J Infect Public Health. 2024;17(6):975–85.
- Murad A, Faruque F, Naji A, Tiwari A, Qurnfula
E, Rahman M, et al. Optimizing health
service location in a highly urbanized city:
multi-criteria decision making and P-Median
problem models for public hospitals in Jeddah
City, KSA. PLoS ONE 2024;19(1):e0294819.
- Alhomaidhi A. Geographic distribution of
public health hospitals in Riyadh. Saudi
Arabia Geogr Bull. 2019;60(1):25–48.
- Al-Sheddi A, Kamel S, Almeshal AS, Assiri AM.
Distribution of primary healthcare centers
between 2017 and 2021 across Saudi Arabia. Cureus
2023;15(7):e41932. https:// doi. org/ 10. 7759/
cureus. 41932.
- Al Saffer Q, Al-Ghaith T, Alshehri A, Mohammed
R, Homidi S, Hamza MM, et al. The
capacity of primary healthcare facilities in
Saudi Arabia: infrastructure, services, drug
availability, and human resources. BMC
Health ServRes 2021;21(365). https://doi.org/10.1186/s12913-021-06355-x.
- Acharya S. The challenges of healthcare
delivery in low-resource settings. J
Intensive Crit Care Nurs 2023;6(5):172
- Alharthi NA, Alharthi TH, Alzaidi AM,
Althobaiti SW, Alosimi MM, Hummadi MA et al.
Addressing the nursing workforce shortage in
Saudi Arabia: a multi-faceted approach. Migrat.
Lett. 2022;19 S5(2022).354-359.
- Michaeli DT, Michaeli JC, Albers S, Michaeli
T. The healthcare workforce shortage of nurses
and physicians: practice, theory, evidence, and
ways forward. Policy Politics Nurs. Pract. 2024;25(4):216-227.
|




