|
Introduction
Oncocytic carcinomas
are rare malignant salivary gland tumor most
commonly involving major salivary glands. They are
epithelial tumors defined by the presence of
abundant eosinophilic granular cytoplasm due to
high mitochondrial content. Although most commonly
identified in the major salivary glands, oncocytic
carcinomas may also arise in minor salivary gland
tissue in anatomic subsites of the head and neck,
including the paranasal sinuses, nasolacrimal
system, and nasopharynx. They can also arise in
other organs, including the kidney, breast,
prostate gland (1).
Case Report
A 65 year old
gentleman presented with right nasal blockage
since 5 months in the outpatient department of
head and neck surgical oncology, Malabar cancer
centre, Thalassery. Clinical history revealed
epistaxis of 4-5 episodes since 2 months and
anosmia. He had hypertension along with coronary
artery disease for which he underwent percutaneous
transluminal coronary angioplasty 4 years back. On
clinical examination there was no proptosis, loss
of visual acuity, cheek swelling, headache, and
eye movements were normal. Oral cavity and
ophthalmic examination were unremarkable. Nasal
Endoscopy revealed a tumour in the right nasal
cavity, extending to middle meatus involving
middle turbinate, medial wall of maxilla, inferior
turbinate extending to sphenoethmoidal recess and
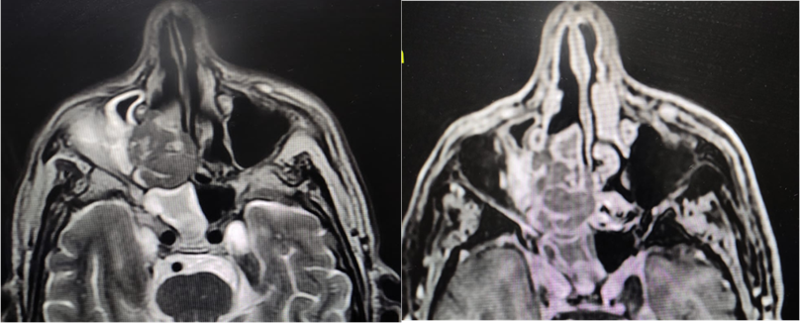
eroding posterior part of septum. MRI, head and
neck showed a polypoidal 46 x 39 x 27 mm lesion
involving right nasal cavity infiltrating the
nasal septum, eroding medial wall of maxilla with
suspicious erosion of cribriform plate with no
involvement of dura (Figure 1,2). CT Thorax and
abdomen done for metastatic workup was normal.
|
| Figure
1: A Polypoidal 46 x 39 x 27 mm lesion
seen involving right nasal cavity.
Infiltrating the nasal septum, eroding
medial wall of maxilla, suspicious erosion
of cribriform plate, dura appears free.
|
|
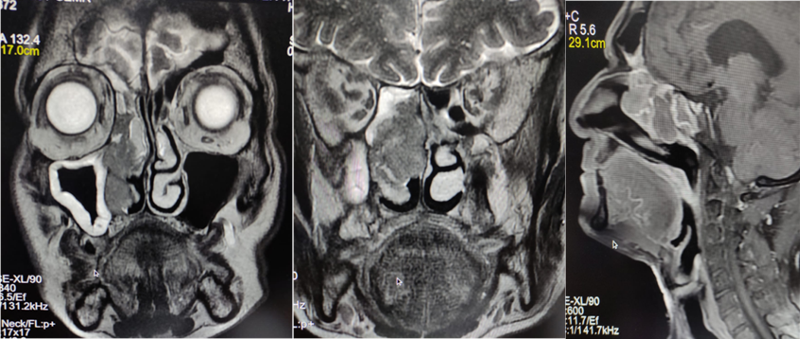
| Figure
2: Mucosal thickening with fluid seen
within the right maxillary sinus, ethmoid
sinus, right frontal sinus and sphenoid
sinuses. |
An endoscopic biopsy
was performed which showed sheets of large cells
with abundant eosinophilic granular cytoplasm. The
differential diagnosis considered were oncocytic
carcinoma, secretory carcinoma and mucoepidermoid
carcinoma with oncocytic change. Endoscopic
craniofacial resection of sinonasal mass was done
and margins were cleared laterally up to lamina
papyracea, medially up to nasal septum, inferiorly
up to the mucosa of floor of nasal cavity and
superiorly to the cribriform plate. Skull base
defect were repaired with fascia lata, fibrin glue
and nasoseptal flap. The margins and the excised
tumor were sent for histopathological examination.
The patient received adjuvant radiotherapy and he
is under regular follow up.
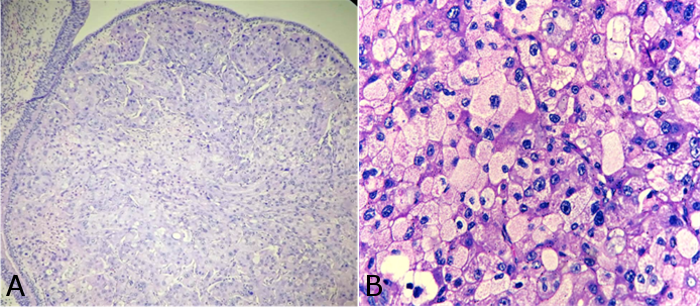
Microscopic
examination revealed an infiltrative neoplasm with
tumor cells arranged in sheets, nests and lobules.
The individual tumour cells (oncocytes) were large
in size with hyperchromatic, pleomorphic nuclei
and have prominent nucleoli with eosinophilic
granular cytoplasm. Tumor showed mitotic activity
of approx. 18-20/10hpf. All the resection margins
were found free of tumor.
|
| Figure
3: H and E stained section showing
oncocytic cells arranged in sheets [4x(A),
40x(B)] |
Discussion
Oncocytic carcinoma
of salivary gland origin is an extremely rare
tumor composed of malignant oncocytes showing
infiltrative qualities, including local invasion,
regional or distant metastases(2). Most of the
case are reported in major salivary glands. Only a
few cases have been reported in nasal cavity.
Compared with oncocytomas arising from major
salivary glands, those that arise elsewhere from
minor salivary glands tend to be more locally
aggressive with greater malignant potential,
classified as oncocytic carcinomas.(3)
Most of the reported
cases of sinonasal oncocytic carcinomas have a
male predilection and age>60 years.The
clinical presentation of this case is in
concordance with the previously reported cases in
English literature. Owing to the granular
cytoplasm of tumor cells, the histopathological
differentials considered were oncocytic carcinoma,
oncocytic subtype of mucoepidermoid carcinoma and
secretory carcinoma with oncocytic changes. Mucous
cells were not identified which ruled out
oncocytic subtype of mucoepidermoid carcinoma.
Also immunohistochemistry for mammaglobulin was
negative in this case.
| Table 1: Reported
cases of sinonasal oncocytic carcinomas in
literature. |
|
Author
|
Patient
|
Location
|
Treatment done
|
|
Abe et al, 2007(4)
|
47/male
|
Nasal cavity
|
Endoscopic medial maxillectomy+ modified
radical neck dissection +Adjuvant
radiotherapy
|
|
Chui et al, 1985(5)
|
58/female
|
Nasal cavity
|
Lateral rhinotomy
|
|
Cohen and Batsakis,1986(6)
Johns 1973(7)
|
61/male
|
Nasal cavity, paranasal sinuses and
orbit.
|
Medial maxillectomy - Caldwell-Luc
approach.
|
|
Corbridge et al, 1996(8)
|
78/female
|
Nasal cavity, paranasal sinuses
|
Lateral rhinotomy.
|
|
DiMaio et al,1980(9)
|
32/male
|
Nasal cavity and paranasal sinuses
|
Local excision +Adjuvant radiotherapy
|
|
Hu et al, 2010(10)
|
73/male
|
Nasal cavity initially, paranasal sinuses
|
Lateral rhinotomy+Adjuvant radiotherapy
|
|
Jung et al, 2013(11)
|
64/male
|
Nasal cavity and paranasal sinuses
|
Endoscopic inferior medial maxillectomy +
Dacryocystectomy+adjuvant radiotherapy
|
|
Mikhail et al,1988(13)
|
84/female
|
Nasal cavity
|
Radical maxillectomy and orbital
exenteration
|
|
Nayak et al,1999(14)
|
50/female
|
Nasal cavity
|
Extended medial maxillectomy via lateral
rhinotomy +Adjuvant radiotherapy
|
|
Perlman et al,1995(15)
|
80/male
|
Lacrimal sac, paranasal sinuses
|
Caldwell-Luc approach +Adjuvant
radiotherapy
|
|
Savic et al, 1989(16)
|
45
|
Nasal cavity and paranasal sinuses
|
Excision via Denker procedure
|
|
Beegum F etal 2023
|
65/male
|
Right nasal cavity, middle turbinate,
medial wall of maxilla, inferior
turbinate, sphenoethmoidal recess
|
Endoscopic resection+adjuvant
radiotherapy
|
Sinonasal oncocytic
carcinomas are more likely to be malignant
compared to that occurring in major salivary
glands with more frequent local invasion and
recurrence. Regarding treatment of sinonasal
oncocytic carcinomas, several surgical approaches
have been reported in literature. Surgical
excision is the main modality of treatment. The
major limitation of reported cases of sinonasal
oncocytic carcinomas in literature is the lack of
information regarding status of resection margins.
Endoscopic approach offers easy access to both the
nasal cavity and nasolacrimal apparatus and
provide excellent visualization. The success of
endoscopic approach depends on experience of the
surgical team and optimal preoperative imaging.
The role of adjuvant
radiotherapy in preventing recurrence is
questioned with the suggestion that these tumors
are radioresistant.(12) However, when the disease
is locally advanced, or with regional and distant
metastasis, adjuvant radiotherapy can be a useful
approach to prevent recurrence and spread.(17)
Also, regarding the utility of systemic
chemotherapy for treating sinonasal oncocytic
carcinomas there is insufficient information in
the literature.(18) Finally, a diagnosis of
sinonasal oncocytic carcinoma warrants careful
monitoring and follow-up, as it is locally
destructive and capable of metastasis and multiple
recurrences.(19)
Conclusion
Owing
to the rarity of these tumors, there is no
standard management approach, with several
different surgical techniques reported in the
literature, including both the open and endoscopic
approaches, in addition to variable use of
radiotherapy. Newer technologies may also help the
surgeon to obtain clear surgical margins like
fluorescence guided surgery will better show the
limits of tissue invasion and thus help to define
the surgical margins.
References
- Hamperl H. Benign and malignant oncocytoma. Cancer.
1962;15:1019–1027.
- Hampel H. Onkozyten und Geschwulste der
Speicheldrusen. Virchows Archiv Pathol. 1931;282:724–36.
- Colreavy MP, Sigston E, Lacy PD,
Balasubramaniam GS, Lyons BM. Post-nasal space
oncocytoma: a different approach to a rare
tumour. J Laryngol Otol.
2001;115:57–59.
- Abe T, Murakami A, Nakajima N, et al.
Oncocytic carcinoma of the nasal cavity with
widespread lymph node metastases. Auris
Nasus Larynx. 2007;34:393–396.
- Chui RT, Liao SY, Bosworth H. Recurrent
oncocytoma of the ethmoid sinus with orbital
invasion. Otolaryngol Head Neck Surg.
1985;93:267–270.
- Cohen MA, Batsakis JG. Oncocytic tumors
(oncocytomas) of minor salivary glands. Arch
Otolaryngol. 1968;88:71–73.
- Johns ME, Batsakis JG, Short CD. Oncocytic and
oncocytoid tumors of the salivary glands.
Laryngoscope. 1973;83:1940–1952
- Corbridge RJ, Gallimore AP, Dalton CG, O’Flynn
PE. Oncocytomas of the upper jaw. Head Neck.
1996;18:374–380.
- DiMaio SJ, DiMaio VJ, DiMaio TM, Nicastri AD,
Chen CK. Oncocytic carcinoma of the nasal
cavity. South Med J. 1980;73:803–806.
- Hu YW, Lin CZ, Li WY, Chang CP, Wang LW.
Locally advanced oncocytic carcinoma of the
nasal cavity treated with surgery and
intensity-modulated radiotherapy. J Chin Med
Assoc. 2010;73:166–172.
- Jung JH, Shin DH, Cho KS, Choi HY.
Nasolacrimal duct obstruction caused by
oncocytic carcinoma. Korean J Ophthalmol. 2013;27:126–129.
- Mahmoud NA. Malignant oncocytoma of the nasal
cavity. J Laryngol Otol. 1979;93:729–734.
- Mikhail RA, Reed DN Jr, Bybee DB, Okoye MI,
Dodds ME. Malignant oncocytoma of the maxillary
sinus—an ultrastructural study. Head Neck
Surg. 1988;10:427–431.
- Nayak DR, Pillai S, Balakrishnan R, Thomas R,
Rao R. Malignant oncocytoma of the nasal cavity:
a case report. Am J Otolaryngol. 1999;20:323–327.
- Perlman JI, Specht CS, McLean IW, Wolfe SA.
Oncocytic adenocarcinoma of the lacrimal sac:
report of a case with paranasal sinus and
orbital extension. Ophthalmic Surg. 1995;26:377–379.
- Savic D, Djeric D, Jasovic A. [Oncocytoma of
the nose and ethmoidal and sphenoidal sinuses].
Rev Laryngol Otol Rhinol (Bord).
1989;110:481–483.
- Hoppe BS, Stegman LD, Zelefsky MJ et al.
Treatment of nasal cavity and paranasal sinus
cancer with modern radiotherapy techniques in
the postoperative setting—the MSKCC experience.
Int J Radiat Oncol Biol Phys. 2007;67:691–702.
- Bossi P, Saba NF, Vermorken JB, et al. The
role of systemic therapy in the management of
sinonasal cancer: a critical review. Cancer
Treat Rev. 2015;41:836–843.
- Hodzic Z, Rowan NR, Kashiwazaki R, Willson TJ,
Wang EW, Lee SE. A systematic review of
sinonasal oncocytomas and oncocytic carcinomas:
Diagnosis, management, and technical
considerations. Int Forum Allergy Rhinol.
2017;XX:1–11.
|




