Introduction:
Adolescents are an important resource of any country. According to the Expert committee of World Health Organisation, adolescence is defined as the period between 10-19 years, the second decade of life (1). Adolescents comprise 20% of the world’s total population. Out of 1.2 billion adolescents world-wide, about 85% live in developing countries. In India there are 190 million adolescents comprising 21% of India’s total population (2).
About 16 million girls aged 15 to 19 years give birth every year, accounting for about 11 per cent of all births worldwide. Fifteen per cent of all unsafe abortions in low- and middle-income countries are among adolescent girls aged 15-19 years.(3) In India, birth rate in girls aged 15–19 years is 107 per 1000 girls (1998–99). Adolescent birth rates are intertwined with rates of spontaneous and induced abortions.(4) Adolescence is a significant period for mental, emotional and psychological development. This period represents a window of opportunity to prepare for healthy adult life. In order to lead healthy, responsible and fulfilling lives & protect from reproductive health problems adolescent girls need to be knowledgeable regarding their sexual and reproductive health.
Adolescent girls need adequate information about the physical, psychological changes that take place during puberty, menstruation, pregnancy and child birth. Family formation is a combination of various factors such as girls' ideal age at marriage, ideal number of children and ideal birth interval. Various studies on knowledge, attitude and practice regarding reproductive health issues bring out disturbingly low level of contraceptive awareness among adolescents. The need to address these problems through reproductive health education has been recognized at various national & international forums. This study attempts to look at the knowledge and attitude of adolescent girls of the age group 17-19 years on family formation and reproductive health issues in an urban area of Pondicherry.
Methods
Study site and population: A cross-sectional study was carried out among adolescent girls residing in an urban ward of Puducherry. Ethical clearance for the study was obtained from the Institute ethics committee. Ethical issues involved in the study were less than minimum risk to the study subjects. Permission to carry out the study was obtained from the Anganwadi and the non-formal leaders.
Sample size and sampling: Adolescent girls belonging to the age group of 17 to 19 years and residing in the selected anganwadi service area were included in the study. Married girls in the eligible age group residing in these areas were excluded. Assuming proportion of girls with correct knowledge of age at marriage to be 50%, and precision of 10%, the sample size was calculated to be 97. Assuming 10% non response, final sample size was estimated to be 105. An urban ward was randomly chosen as the site of study from among the various urban areas in Puducherry. Six anganwadis were selected in this area by simple random sampling technique, in order to achieve the sample size. All adolescent girls registered with the anganwadis were included in the study.
Study tool: A structured questionnaire was developed to study the knowledge and attitude regarding the following parameters: family formation - age at marriage, ideal age for marriage, time of first pregnancy, birth spacing; reproductive health issues - contraception, menstrual cycle; child rearing practices - delivery, exclusive breast feeding, supplementary nutrition, immunization. Details of the parents’ occupation, income, educational qualification and family income were also collected. The questionnaire was translated into the local language (tamil) and backtranslated to English, in order to check for validity. It was pretested and revised as per inputs from the pilot study, before using it for study population.
Data collection: Data collection was through house to house survey. Before administering the questionnaire, informed consent was obtained from the parents for girls below 18 years and from the participants above 18 years of age. Confidentiality of the data obtained was ensured. All the participants were explained about the purpose of the study. Data was then collected with help of the questionnaire.
Statistical analysis: Data were entered into Microsoft excel spread sheet. Data analysis was carried out using SPSS 16.0. Mean, Standard deviation and proportions were calculated.
Results
A total of 120 girls were approached and response rate was 100%. Among the study subjects, around half of them were 17 years of age, while 34% and 21% were aged 18 and 19 years respectively. Majority of them (80%) were doing their higher secondary while the rest of them were in college.
Table 1: Knowledge and awareness of the respondents on family formation and child care practices |
Domains |
Aware n (%) |
Not aware n (%) |
Family formation |
Contraceptive methods |
11 (9.2) |
109 (90.8) |
Emergency contraception |
6 (5) |
114 (95) |
Safe period during menstruation |
8 (6.7) |
112 (93.3) |
Small family norm |
107 (89.2) |
13 (10.8) |
Spacing |
54 (44.9) |
66 (55.1) |
Government welfare schemes for pregnant women (JSY) |
88 (73.3) |
32 (26.7) |
Child care practices |
Exclusive breastfeeding |
41 (34.2%) |
79 (65) |
Supplementary feeds |
29 (24.2) |
88 (73.3) |
Immunisation for children |
99 (82.5) |
21 (17.5) |
One fifth (21%) and one third (31%) of the study subjects knew the legal age for marriage to be 21 years for boys and 18 years for girls respectively. One third of the subjects felt that the desirable age for marriage in boys and girls should be between 21-25 years.
Majority (89%) of girls were aware of the small family norm. When asked about the ideal family size, 88% subjects responded as two children, followed by 11% who responded as single child. Regarding the age of the mother during her first pregnancy, 85% of the girls considered that 20-25 years was the ideal age while 7.5% perceived 26-30 years as a favourable time; rest of them were uncertain about this age. All the respondents were aware about the need for spacing between the first and second child, and almost half of them (45%) responded that the gap should be more than 2 years.
Awareness on contraception was poor among the study population. Only 9% (n=11) of the girls were aware of any contraceptive method. Six subjects were aware about oral contraceptive pills, while 3 subjects were aware of condoms and copper T as contraceptive methods; only one subject was aware about tubectomy. Only 5% know about emergency contraception. On exploring the attitude of the respondents about the use of contraceptive methods after marriage, around 38% of the subjects considered family welfare measure to be important for a healthy family, while 56% were against the use of contraception.
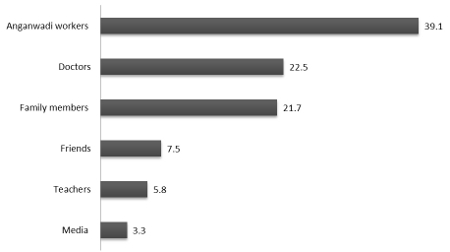 |
Figure 1: Source of information about maternal and child health practices among the study population |
Regarding the food items that should be included in the diet of pregnant women, 78% subjects considered fruits and vegetables as essential. Some subjects gave specific responses like spinach (47%), pulses (19%), milk (17%), eggs (8%), fish (3%), vitamin tablets (3%), vitamin A (2.5%) and iodised salt (2%). Around 10% subjects were not aware about the dietary requirements during pregnancy. In order to find out the taboos regarding diet, the girls were asked to name food items that should be avoided during pregnancy. Majority of the girls mentioned papaya (65%) and pineapple (25%). Some of the other responses were oily food (12%), fastfood (8%), sesame seeds (7%). Nearly 73% subjects were aware of the monetary benefits for pregnant women provided by the government under Janani Suraksha Yojana.
About 98% of the girls were aware that breast milk was the ideal food for babies. Only 34.2% of the girls were aware of exclusive breast feeding. One fourth of the girls (24.2%) had a good understanding on supplementary feeding. Majority (89%) of the girls were aware that immunization is essential for infants. To understand their knowledge about the basic vaccines, the respondents were asked to name a few vaccines the child would receive in the first year of life. Forty percent of them mentioned BCG, followed by polio (38%) and rubella (20%). Few subjects were also aware of vaccines like measles (13.3%), DPT (10.8%) and chicken pox (15%), MMR (5%), Japanese Encephalitis (3.3%) and Hepatitis (5.8%). Less than 20% of the subjects were not aware of any vaccine available for children. More than two-thirds of the subjects considered Sub centre and Primary Health Centre as the best health facility for receiving vaccination. Government hospital was mentioned by 28% of the subjects, while two subjects felt that private clinics were better for immunization.
Anganwadi workers were the important source of information on reproductive health and family welfare issues for around 40% of the subjects, followed by doctors (22%) and family members (22%). The other sources of information were media (3%), teachers (6%) and friends (7.5%).
Discussion
This study aimed to elicit the knowledge and attitudes of adolescent girls in Pondicherry on family formation and reproductive health issues. In India, the legal age of marriage is 18 years for girls and 21 years for boys. Only one third of the girls knew the legal age for marriage among girls, while 22% were aware of the legal age for marriage among boys. This is very less when compared to studies done in other parts of the country.(5) Girls who enter into marriage early face serious health risks; being married, they are more likely to be exposed to frequent, unprotected sex compared to their unmarried peers, and hence more vulnerable to adverse pregnancy outcomes, HIV infection and violence. Hence, the legal age of marriage for both boys as well as girls should be emphasised at the adolescent age level itself, and they must be aware of their rights. Puducherry being a literate state, women’s education is given due priority. By default, majority of the girls enter college education and therefore this may be the reason for low awareness of legal age (as 18 years) among the adolescent girls. This is also reflected by the fact that 74% of the adolescent girls in this study were in favour of marriage after 18 years of age. Girls probably prefer a later age for marriage because they may want more opportunities for their own education and employment before marrying and increase their leverage in the decision making process.
Understanding about the small family norm was good among the study population. In our study, 89.2% responses were in favour of a two-child family. An earlier study done in Puducherry reported that 76% of girls were in favour of the 'two-child norm'.(6) Similar findings were also reported in the study done among the adolescent girls in Haryana.(7) Majority of the studies have reported that women consider a small or moderate size family as ideal rather than a very large one. If the fertility preferences of adolescent girls can be moulded to adopt the small family norm, considerable progress can be made towards achieving the population goals.
All the respondents were unanimous in their desire for a gap between the first and second child, with half of them (45%) preferring a gap of more than two years between the children. This is slightly lower when compared with the study done in Ludhiana which showed that 62% of the adolescent girls preferred a gap of more than 2 years between the pregnancies.(5)
The awareness on contraceptive methods was very low in this study (only 9.2%). Furthermore only 5% of the girls were aware about emergency contraception. When questions were asked about the use of contraception after marriage, 37.5% of the girls were for the use of contraception while a majority of 55.8% were against the use of contraception and the rest were ambivalent. This could be attributed to the lack of awareness about family planning, therefore highlighting the need for sex education and reproductive health programmes for young adults. Another reason could be the social taboos around the discussion of issues related to family planning by young women whether married or unmarried.
Young women are less likely than their older counterparts to use modern contraceptives. On one hand married adolescents may feel social pressure to bear a child and thus not seek family planning services, and on the other hand unmarried adolescent girls face a different type of social pressure, fearing judgment or dealing with a socially-unsanctioned pregnancy. Increasing their vulnerability, some adolescent girls are subject to sexual exploitation and abuse, and many have limited knowledge about how to protect their health.(8) Education and motivation of the adolescents will go a long way in influencing their reproductive attitudes and behaviour, which in turn is likely to have an important impact on overall reproductive health, demographic and social outcomes.
Majority of the girls considered fruits and vegetables essential during pregnancy and they were able to identify nutritious foods for pregnancy. This clearly indicates that these girls already have prior knowledge about the dietary habits during pregnancy. However, the study also identified certain food taboos being prevalent from adolescent age of the girls (eg. avoidance of pineapples, papayas).
Anganwadi workers were the important source of information for the majority of girls followed by doctors. Given the social taboos often surrounding puberty and hesitance to discuss issues regarding family formation, it is particularly important to give adolescents the required information through some formal channel.
Currently, the government is reaching out to adolescent girls by involving teachers and health workers through pilot programs in ICDS (Integrated Child Development Services), Village Health and Nutrition Days and specific programs targeting adolescent girls like WIFS (Weekly iron folic acid supplementation programs). The Ministry of Women and Child Development, Government of India, in the year 2000 came up with scheme called “Kishori Shakti Yojna” (KSY) using the infrastructure of ICDS. Rajiv Gandhi Scheme for Empowerment of Adolescent Girls (RGSEAG) -“SABLA” would replace KSY and NPAG in the 200 selected districts. The objectives of the Scheme are to enable the adolescent girls for self-development and empowerment through promoting awareness about health, hygiene, nutrition, Adolescent Reproductive and Sexual Health (ARSH) and family and child care.(9) Age appropriate guidance in two groups of 11-15 and 15-18 are provided on various topics under the scheme (Table 2).
Table 2: Content of Education, Counseling and Guidance services under the SABLA scheme (9) |
Nutrition and Health Education |
Healthy cooking and eating habits, safe drinking water, balanced diet, locally available nutritious food, nutrition deficient disorders, their prevention, nutrition during pregnancy and infancy, IYCF, etc |
Personal hygiene, sanitation, onset of puberty and related changes, exercise, yoga, first-aid, harmful myths and traditional practices, home remedies, common ailments, avoiding drugs and alcohol abuse, stress management ,etc. |
Adolescent and Reproductive |
Age specific modules for adolescent and reproductive sexual health, onset of puberty, menstrual hygiene, planned parenthood, AIDS/HIV/STD, contraception etc. |
Family Welfare |
Family planning, reproductive cycle, benefits of marriage and children at right age, safe motherhood, immunization etc. |
Child care practices |
Healthy child feeding practices, benefits of exclusive breast feeding, handling children, common ailments etc. |
Home management |
Home maintenance, budgeting, saving, running household, gender sensitivity, importance of schooling of children, etc. |
Life Skill education |
Problem solving, critical thinking, communication skills, self-awareness skills, coping with stress and leadership |
Guidance on accessing public services |
Health centers, banks, post offices, Police Station, etc. |
Conclusion and recommendations:
Young individuals are growing in number and yet they are the most deprived generation when it comes to access to information, services and policy recommendations. In this study, adolescent girls were aware regarding legal age at marriage, small family norm and dietary care during pregnancy. However, knowledge levels on contraceptive measures, exclusive breast feeding and supplementary feeding is less than satisfactory. These gaps in knowledge on reproductive health and family formation need to be addressed. Innovative ways of providing this information in a non-threatening environment that allows adolescents to raise their own concerns need to be encouraged at the school and community levels. As comprehensive education programs like SABLA are functioning in pilot districts, universal coverage can be aimed through sustainable programs. Health workers can be trained to impart this knowledge through adolescent clinics at Primary Health Centres. Similarly, school teachers can be trained and suitable topics can be included in the school curriculum.
References
- The second decade: Improving adolescent health and development. World Health Organisation, Geneva: WHO, 2001: 1-20.
- Malleshappa K, Krishna S, Nandini C. Knowledge and attitude about reproductive health among rural adolescent girls in Kuppam Mandal: An intervention study. Biomedical Research. 2011;22(3):305–10.
- UNFPA. From childhood to womanhood: meeting the sexual and reproductive health needs of adolescent girls. Available from: http://www.unfpa.org/sites/default/files/resource-pdf/EN-SRH%20fact%20sheet-Adolescent.pdf Cited on Oct 5, 2014.
- Bearinger LH, Sieving RE, Ferguson J, Sharma V. Global perspectives on the sexual and reproductive health of adolescents: patterns, prevention, and potential. Lancet. 2007 Apr 7;369(9568):1220–31.
- Benjamin AI, Panda P, Singh S, Bhatia AS. Knowledge & Attitude of Senior Secondary School Students of Ludhiana Regarding Population Control & Contraception. Ind J Comm Med. 2001;26(4):10–12.
- Srinivasa K, Sahai A, Ramalingam G, Premarajan KC. Knowledge and perception of adolescents regarding factors affecting family formation. Journal of Family Welfare 1993 Dec; 39(4):47-5.
- Pattanaik D, Lobo J, Kapoor SK, Menon PS. Knowledge and attitudes of rural adolescent girls regarding reproductive health issues. Natl Med J India. 2000 Jun;13(3):124–8.
- UNFPA and Guttmacher Institute. Adding it Up: The Costs and Benefits of Investing in Family Planning and Maternal and Newborn Health. 2009. [Internet]. Available from: http://www.guttmacher.org/pubs/AddingItUp2009.pdf. Cited on Oct 5, 2014.
- Ministry of Women and Child Development, Government of India. Rajiv Gandhi scheme for empowerment of adolescent girls (RGSEAG) ‘SABLA’ - The scheme. Available from: http://wcd.nic.in/SchemeSabla/sablaguidemar11.pdf
|

